Published in John Menadue – Pearls and Irritations, 12 June 2020
Australia’s response to coronavirus to date has been among the most successful in the world. After an exponential increase that peaked at more than 400 cases a day in late March, daily cases declined to about 20 a month later, with some states recording several successive days or weeks with no new cases. At the same time, rapid growth in infections in almost every other comparable country threatened to overwhelm their health systems.
As Australia eases its restrictions, it is time to reflect on what was successful and where Australia could have done better. These lessons should inform the next stage of Australia’s response as we transition to a new normal.
Four successes
Australia has avoided the worst of the pandemic (at least for now). Comparable countries, such as the U.K. and U.S., are mourning many thousands of lives lost and are still struggling to bring the pandemic under control. The reasons for Australia’s success story are complex, and success may yet be temporary, but four factors have been important.
Success 1: Cooperative governance informed by experts
The formation of a ‘National Cabinet’, comprising the Prime Minister and the leaders of each state and territory government, was a key part of Australia’s successful policy response to COVID-19.
The states and territories have primary responsibility for public hospitals, public health, and emergency management, including the imposition of lock-downs and spatial distancing restrictions. The Commonwealth has primary responsibility for income and business support programs. Coordination of these responsibilities was critical.
The National Cabinet was created quite late – in mid-March when cases were beginning to increase exponentially – it has proven to be an effective mechanism to resolve most differences and coordinate action as much more dramatic and far-reaching measures were put in place.
Within a week of the National Cabinet being formed, Australia began to progressively implement restrictions on social gatherings. On 22 March, in advance of a National Cabinet meeting that evening, Victoria, NSW, and the ACT announced they were proceeding in the next 48 hours to implement a shutdown of all non-essential activity. This helped push all other governments into widespread business shutdowns announced by the Prime Minister that night, to take effect the following day.
National cooperation was further enhanced by the inter-jurisdictional Australian Health Protection Principal Committee (AHPPC). From the start of the crisis, this forum helped underpin Australia’s decisions with public health expertise. The AHPPC’s recommendations informed government decisions, particularly the expansion of spatial distancing measures. It is now commonplace to have the Prime Minister give a national press briefing alongside the Chief Medical Officer, who chairs the AHPPC.
The Commonwealth Government was criticised, however, for announcing it was suspending Parliament. While the Commonwealth was making significant national decisions, including record spending commitments, the suspension meant the Government had minimal formal oversight. To at least partially overcome this deficiency, on 8 April the Senate set up a select committee to provide some checks and balances on the Government’s response.
Success 2: Closure of international borders and mandatory quarantine
Australia’s decision to close its borders to all foreigners on 20 March to ‘align international travel restrictions to the risks’ was a turning point in Australia’s response. The overwhelming number of new cases (about 90 per cent) during the peak of the crisis came from or were directly linked to someone who had been overseas.
This marked the start of Australia’s ‘escalated national action’ phase. Within two weeks of Australia’s borders being closed to foreigners, Australia’s daily case numbers began to fall.
And once this measure was coupled with mandatory quarantine at designated facilities for all Australian international arrivals a week later, Australia had much more control over the spread of the virus.
Success 3: Rapid adoption and acceptance of enhanced spatial distancing measures
Australia’s rapid adoption of spatial distancing measures reduced the risk of community transmission.
Over February, COVID-19 cases were rapidly spreading in countries beyond China, reaching at least 75 countries worldwide by 2 March. Italy was particularly hardest hit, overtaking China’s death toll by mid-March. In the most affected regions of Italy, the health system was close to collapse. Once Australians could see the risk of the virus overwhelming the nation’s health system, highlighted by Italy’s struggling health system at the brink of collapse, people quickly complied with shutdown laws. In fact, Australians had already begun reducing their activity before the restrictions were imposed.
Australians’ successful compliance is demonstrated by the low number of community transmissions, despite having less-strict lockdown laws than some other countries such as France and New Zealand.
Success 4: Expansion of telehealth
One of the Commonwealth’s early healthcare interventions was to radically expand Australians’ access to telehealth. Telehealth enables patients to consult health professionals via video-conference or telephone, rather than face-to-face. This means that healthcare workers and patients can remain home rather than put themselves into a higher-risk setting such as a healthcare clinic or a doctor’s waiting room.
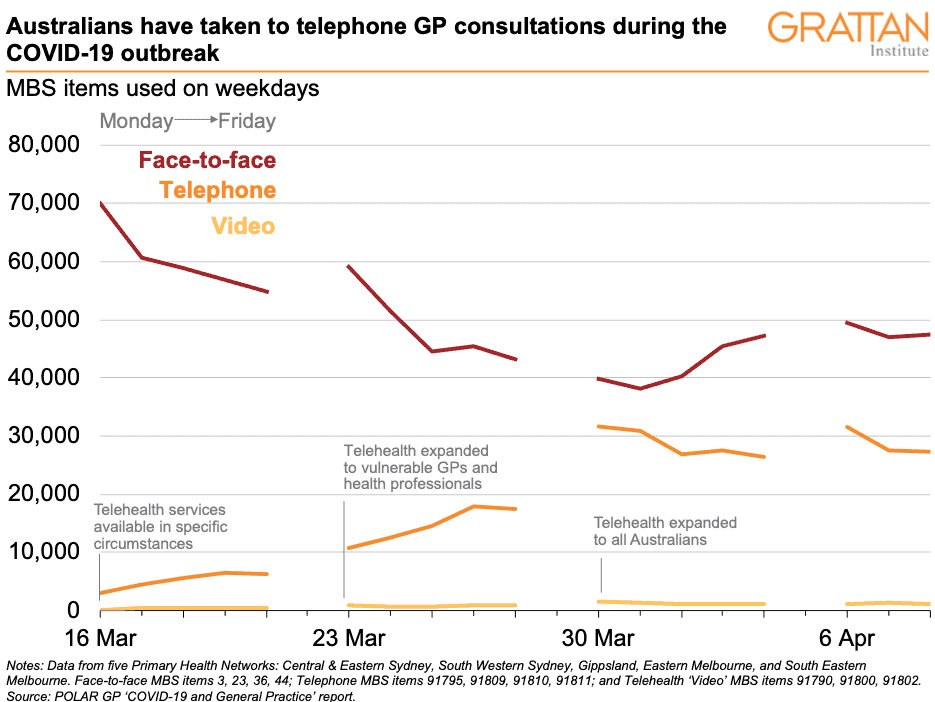
The Commonwealth announced the first of these measures in its $2.4 billion health package on 11 March, and quickly phased-in broad-scale telehealth services for all Australians. Within six weeks, over 250 new ‘temporary’ items had been added to the Medicare Benefits Schedule, which extends to seeking advice from allied health workers and specialists. These changes were complemented with changes to medication services, enabling electronic delivery of prescriptions to the pharmacy, with options for patients to have medications delivered to their homes.
Australians have enthusiastically taken up telehealth services, with more than 4.3 million medical and health services delivered to three million patients in the first month. In fact, a RACGP survey of over 1,000 GPs found that 99 per cent of GP practices were now offering telehealth services, with 97 per cent also continuing to offer face-to-face consultations.
Four failures
Unfortunately, Australia has also had failings. The most obvious is the handling of the Ruby Princess cruise ship, but Australia might have been in a better position today if it had acted against the virus more quickly and if our leaders had been clearer about where they were headed.
Australia eventually ‘went hard’, but it was too slow to get started. The Commonwealth Government spent too long in the early days flailing in uncertainty about the scale of the crisis. As a result of this hesitancy, the Government was too slow to shut international borders and to prepare the healthcare system for the possibility of a huge influx of COVID-19 patients.
Failure 1: The Ruby Princess
About 2,700 Ruby Princess passengers were allowed to disembark freely in Sydney on 19 March, despite some showing COVID-19 symptoms. The cruise ship has become Australia’s largest single source of infection. Nearly 700 cases (about 10 per cent of Australia’s cases) and 22 deaths (about 20 per cent of Australia’s deaths) are linked to the ship.
On 15 April, NSW launched a Special Commission of Inquiry to investigate what went wrong and on 5 May a Commonwealth Senate Select Committee on COVID-19 inquired into the case. NSW police will also spend the next six months investigating what was known about the potential coronavirus cases before the Ruby Princess was allowed to dock.
Failure 2: Too slow to close the borders
Australia spent too long in the uncertainty phase during the early stages of the crisis. While Australia was comparatively quick to ban foreign nationals coming from China, it was slow to introduce any further travel restrictions.
As the virus spread worldwide, and Australia continued to have thousands of international arrivals each day, it took more than six weeks after Australia’s first confirmed case for the Government to introduce universal travel restrictions – first requiring self-isolation for all international arrivals (on 15 March), followed by the borders closing to foreign arrivals (on 20 March). Before this, travel restrictions were targeted at specific countries (e.g. South Korea, Iran and Italy) in an inconsistent way, despite some other countries such as the U.S. posing a similar or greater risk.
Failure 3: Too slow to prepare the health system
Australia was too slow to prepare the health system in advance of the pandemic rapidly spreading in Australia. The initial focus on containment, followed by caution and uncertainty, distracted governments from preparing their health systems early.
This meant that when cases began to rise exponentially, Australia was not fully prepared for a pandemic-scale response. This was particularly evident in Australia’s testing regime. At first, some people with symptoms went to community GP clinics or hospitals, putting others at risk. On 11 March the Commonwealth Government announced 100 testing clinics would be established, but this was only completed two months later, once the peak of the crisis had passed.
As cases began to increase in mid-March, Australia very quickly hit supply shortages for testing. The testing regime remained narrow for too long before new testing kits could be acquired. This meant that many people with symptoms could not be tested, increasing the chances of community transmission. Broader community testing, led by state governments, did not begin until April.
Australia also struggled to get enough personal protective equipment (PPE) quickly enough to meet demand. Australia’s initial national stockpile of 12 million P2/N85 masks and 9 million surgical masks was not enough. Supplies of gowns, visors, and goggles had also not been set aside in Australia’s national stockpile in the event of a crisis. General practitioners complained of inadequate supplies hampering their work. Eventually, on 26 March, elective surgery was severely curtailed so that PPE could be diverted to frontline health workers dealing with the pandemic.
As shortages loomed, Australian health departments joined global bidding competitions for fast-track supplies from overseas manufacturers. Some state governments turned to local manufacturers to boost supplies.
Failure 4: Shifting strategies and mixed messages
The lack of a clear overarching strategy to respond to the crisis has resulted in a reactive policy approach. This has led to mixed and confusing messages.
At first, there was confusion about the shutdown measures: which businesses or events should close (for example, the Grand Prix). There have been inconsistencies between the Commonwealth’s position and the states’. For example, most states closed or partially closed their public schools around Easter and began re-opening them when cases went down over a month later. Despite concerns raised by some state governments, the Commonwealth asserted children were not at risk, with the Prime Minister repeatedly encouraging parents to send their children to school. Childcare centres also remained open.
The mixed messages have been particularly pronounced on Australia’s strategy to manage the virus. Initially, the Commonwealth Government talked about ‘slowing the spread’, but some states argued for a ‘stop the spread’ strategy. This tension increased confusion about how far Australia’s lockdown restrictions should go. Debate raged between people who argued that ‘herd immunity’ was Australia’s only option, and people who pushed for ‘elimination’ of COVID-19 in Australia.
When clarity was sought from the Commonwealth, the messaging remained unclear. Even a 16 April statement from the Prime Minister, designed to clarify the Commonwealth’s position on its longer-term strategy, confused two different strategies as one, by saying Australia was continuing to ‘progress a successful suppression/elimination strategy for the virus’.
But even as the debate raged on, the case count forged its own story, showing that elimination may be possible as more and more states began to record multiple days and weeks with no new cases.
And now moving forward
As Australia shifts from crisis mode to recovery mode, there is much uncertainty for the future. How will our governments translate their short-term success in fighting the virus into long-term success in building a post-pandemic Australia?
One thing is certain: Australia’s response to the COVID-19 crisis shows that good decision-making is now more important than ever.