Why are we still waiting for cheaper medicines?
by Peter Breadon, Wendy Hu
Labor has committed A$690 million over four years to cut the maximum cost of medicines on the Pharmaceutical Benefits Scheme (PBS) to $25. The Coalition has matched the promise, which is estimated to save Australians $200 million a year.
But consumers could save even more if an existing policy met its potential.
In 2023, the federal government introduced 60-day prescribing. This meant consumers could get twice as many pills per script, with fewer trips to the pharmacist (and to the doctor for a script).
The government announced that consumers would save up to $190 a year for a single medicine, and up to $46 for a concession card holder, compared to the costs of a 30-day script.
But after a tough fight to get this policy, it isn’t living up to its promise.
A hard-won policy
It took political courage, and government spending, to get this change.
Data on political donations show pharmaceutical interests make up the vast bulk of donations from the health sector. The Pharmacy Guild, which represents pharmacy owners, spent the most by far. These donations are an attempt to wield influence behind the scenes. When that fails, the guild isn’t afraid to attack governments in public.
The federal government stared down a histrionic scare campaign against 60-day prescribing. The guild claimed pharmacies would close due to reduced dispensing fees. It also claimed medicines would run out, and children would overdose due to pill hoarding.
The government pushed through the policy, but directly compensated rural pharmacies with ongoing payments worth $20 million a year.
The government also brought forward negotiation of the eighth Community Pharmacy Agreement, which sets how much the government pays pharmacists for dispensing, medication management, and other services. The agreement was signed last year and added $3 billion in new spending.
A long wait for longer scripts
After all that conflict and cost, our analysis of PBS data shows the uptake of longer scripts has been painfully slow.
About 300 drugs for chronic health conditions have been added to the eligibility list in three stages.
For the first stage of medicines, the 60-day option became available in late 2023. This included common medications such as statins for high cholesterol, perindopril for high blood pressure, and alendronate for osteoporosis.
More than a year later, in November 2024, only 30% of eligible stage one medicines dispensed were from a 60-day script.
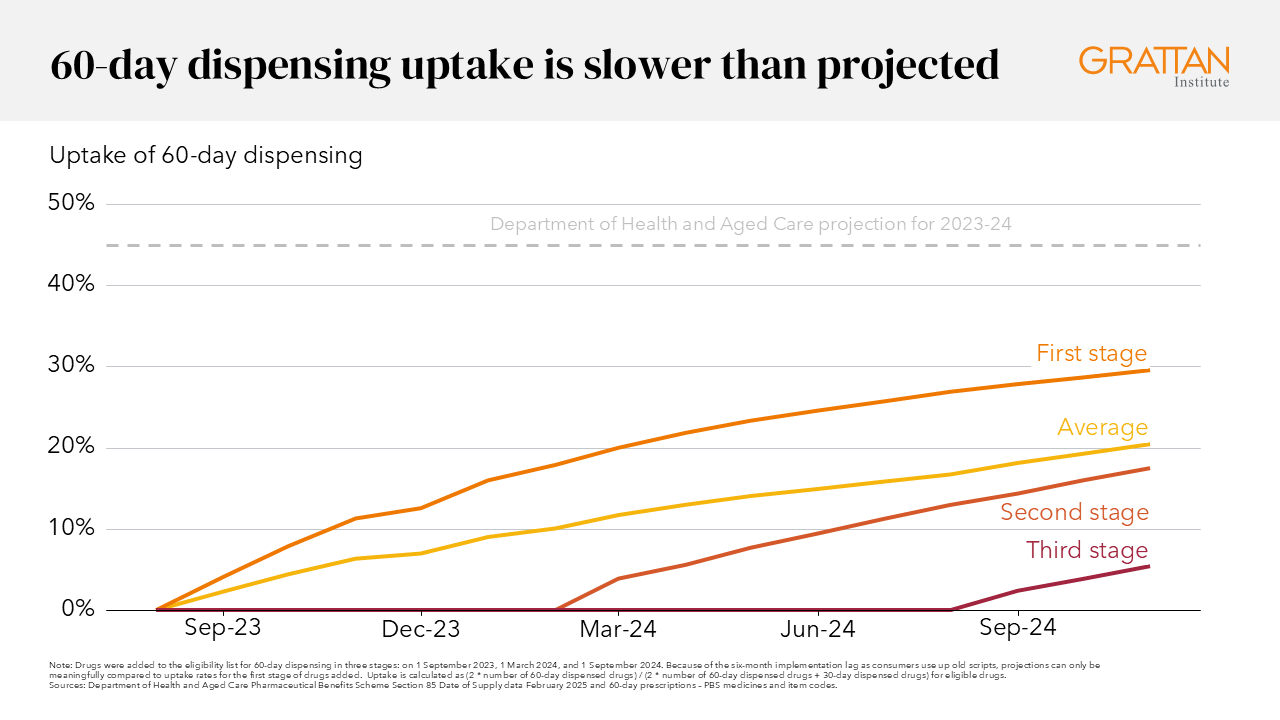
That’s well short of expectations. The Department of Health and Aged Care predicted 60-day uptake would reach 45% in 2023–24, 58% in 2024–25, and 63% in 2026–27, if fully implemented.
Across all medicines eligible for 60-day prescribing, including those added in the second and third stages, just 21% of medicines dispensed were from a 60-day script.
Even at these low rates, we estimate the policy has saved consumers more than $110 million so far. Higher uptake, closer to the rates the department predicted, would mean even more savings.
Millions of people are missing out. In 2024, there were about 28 million 30-day scripts for statins, compared to about 5 million 60-day scripts. If half of these patients had a 60-day script, they would have saved an extra $27 million a year.
If half of all eligible medicines were dispensed for 60 days, we estimate patients would have saved an extra $310 million a year. That’s more than the $200 million in expected savings from the $25 medicines promise.
And while the government spends money on the $25 medicines policy, it saves money from 60-day scripts, by paying pharmacists fewer dispensing fees.
We estimate the government has already saved $141 million from 60-day prescribing. It could save an extra $297 million a year if uptake increased to 50%.
So why aren’t more GPs writing longer scripts?
Despite the Pharmacy Guild’s efforts to undermine the reform, low uptake is more about doctors than pharmacists: the GP who writes the script determines its duration, not the pharmacist.
Risks for patients aren’t the problem. While 60-day prescribing won’t be right for all patients, experts selected the eligible drugs because prescribing them for 60 days is usually appropriate and safe.
While there’s some variation in 60-day prescribing rates for different medicines, it’s low across the board. That suggests the problem isn’t about GPs being much more cautious with some drugs than with others.
The culprit is probably inertia. GP practice software generates default prescriptions when a patient has had a drug before. With most people still getting 30-day prescriptions, that will be the default for most repeat scripts. And many patients might not be aware the new 60-day option is available.
It’s time to get results
With cost-of-living and health system pressures never far from the headlines, making progress on 60-day prescribing should be a priority.
The benefits for patient and government budgets are obvious. But the benefits of freeing up time for busy clinicians shouldn’t be overlooked. Longer scripts means less GP time to write them, and less pharmacist time to fill them.
As Australia gets older and sicker, the need for GP and pharmacist care grows, and there are severe primary care shortages in many parts of the country.
Every second of GP time that can be freed up for diagnosis, treatment, and to help patients manage their conditions is precious.
There is also good evidence pharmacists can provide cost-effective medication reviews, chronic disease management advice and other services. Shifting their time from retail to services is a great way to take pressure off the health system.
So what can be done?
Fortunately, there are some easy shortcuts to longer scripts.
Providers of GP software should make 60-day prescribing the default for relevant medicines.
The Royal Australian College of General Practitioners, the professional body for GPs, should continue to encourage GPs to write longer scripts.
Primary Health Networks, the regional bodies responsible for improving primary care, should tell GPs how they compare with their peers, giving a nudge to GPs with low rates of 60-day prescribing.
Finally, the federal government and consumer groups should run campaigns to inform patients about their options.
Longer scripts are a triple win: savings on medicines for patients, budget savings for the government, and more time for GPs and pharmacists. Few reforms tick all those boxes, so it’s important this one makes its way from good policy to standard practice.