Saving the NDIS: How to rebalance disability services to get better results
by Sam Bennett, Mia Jessurun, Hannah Orban
29.06.2025
report
Chapter
Overview
The National Disability Insurance Scheme (NDIS) is the largest social reform in Australia since the introduction of Medicare. It has transformed the lives of hundreds of thousands of disabled Australians and their families, and been responsible for employing many hundreds of thousands of Australians in the care sector. The NDIS is a vital part of Australia’s social fabric.
But the scheme has grown too big, too fast. The NDIS cost $42 billion in 2023-24 and is expected to cost more than $58 billion by 2028. Growing at about 24 per cent per year on average from 2020-2024, it is one of the fastest-growing pressures on the federal budget and risks crowding out other services that could benefit all disabled Australians.
Design flaws and governance failures baked in from the start have persisted, their impact increasingly stark as costs have spiraled. But more spending has not meant increasingly better results. Most disabled Australians don’t qualify for the NDIS, yet there is little support for them outside the scheme. And the NDIS design is poorly suited to what some people who are currently eligible actually need.
Moderating growth to the 8 per cent by 2026 target set by National Cabinet will not be enough to make the scheme sustainable, and the measures government is relying on to get there risk hitting the target but missing the point.
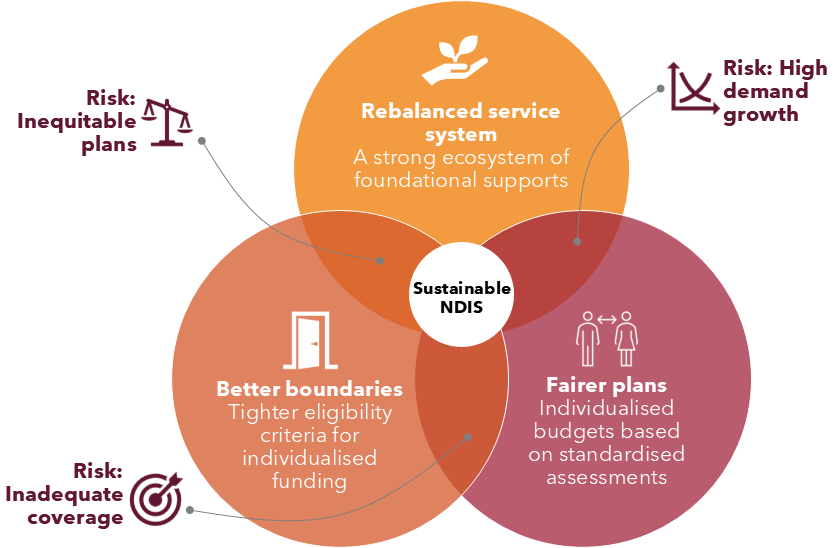
Four big policy changes are needed during this term of federal government to save the NDIS.
First, the NDIS needs clearer, firmer boundaries around who the scheme is for and the needs it is intended to meet, so that the right people receive supports.
Second, the way the NDIS sets budgets and manages claims needs to change so funding is allocated fairly and consistently in a way that is predictable and affordable for governments. People should have more choice and more flexibility in how they use their NDIS funding.
Third, governments should establish a strong tier of ‘foundational supports’ – disability-specific supports outside of individual NDIS packages – to ensure that disabled people get the appropriate supports when and where they need them. This report shows how these services can be delivered by better targeting funding from within the current NDIS budget envelope.
And fourth, Australia needs a new, overarching National Disability Agreement, to clarify the relationship between all aspects of the disability policy landscape and to facilitate cooperation and greater accountability between governments.
This report lays out what governments need to do to save the NDIS without spending more money, and how to ensure this world-leading scheme endures for the good of all Australians, now and into the future.
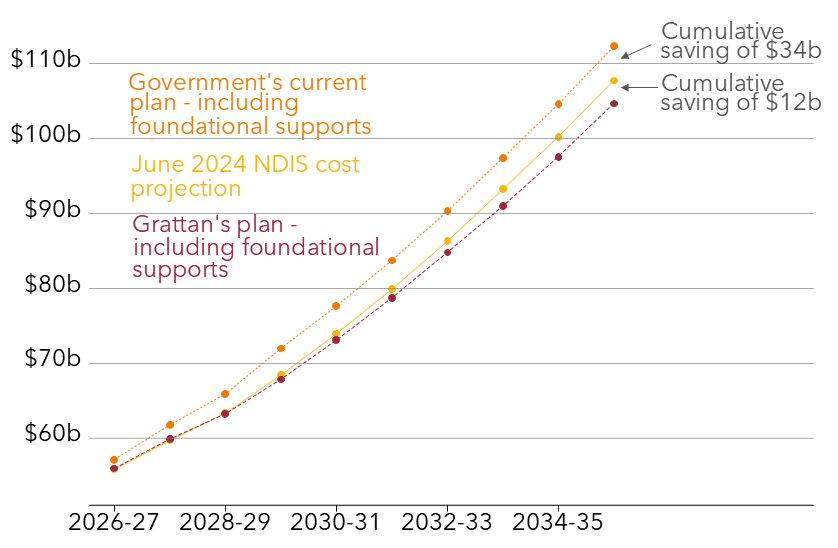
Our plan would deliver three major improvements:
1. A reduction in projected NDIS payments of about $12 billion over the next 10 years, and a further saving of $34 billion over the same period from not requiring new money to fund foundational supports.
2. A more targeted focus for individualised funding and an improved experience for people with the most significant disabilities, who will need the NDIS for their lifetime.
3. A wider net of disability insurance that ensures more disabled people get the help they need in the most efficient and effective way through a range of nationally underwritten, and locally responsive foundational supports.
Recommendations
1. Create firmer boundaries so it is clear who the NDIS is for
Strengthen eligibility criteria for when an impairment should be considered permanent, and include consideration of when the NDIS is the most appropriate service system to meet an applicant’s needs.
Remove diagnosis-based access lists, and design and implement a fair and robust assessment process to determine NDIS eligibility.
Remove the early intervention requirements so that eligible people, especially children with developmental delay or disability, get access to evidence-based, early intervention delivered more effectively and efficiently as targeted foundational supports.
2. Improve claims management to make NDIS plans fairer
Expedite NDIS rule changes to support the adoption of a new needs assessment and budget setting process by July 2026, to incorporate an assessment of function.
Allow people more freedom to plan with support from a wider range of places, including from disabled people’s organisations. The National Disability Insurance Agency (NDIA) should focus planning resources on people with complex needs.
Replace the interim Section 10 Rule with a simpler, more permissive framework that allows people to use their NDIS funds more creatively and flexibly.
3. Use the NDIS budget to fully fund foundational supports
Transition a modest proportion of individualised funding into a new, ambitious tier of foundational supports – delivered within existing government contributions to the NDIS.
Commission targeted foundational supports for children with developmental delay or disability in the places they live, learn, and play, in line with early childhood intervention best practice.
Commission targeted foundational supports for people with psychosocial disability that integrate with existing government services to support their recovery.
4. Improve government accountability for all disability services
Create a new National Disability Agreement to provide a whole-of-system view of disability funding responsibilities and the role of mainstream services, brought up to date to reflect responsibilities for general and targeted foundational supports.
Enable the NDIA to operate more effectively as an insurer and establish a system-wide Sustainability Roadmap covering all services under the new Agreement.
Establish new multi-lateral governance arrangements in each jurisdiction to jointly commission foundational supports that help make the NDIS more sustainable and complement existing services to meet local needs.
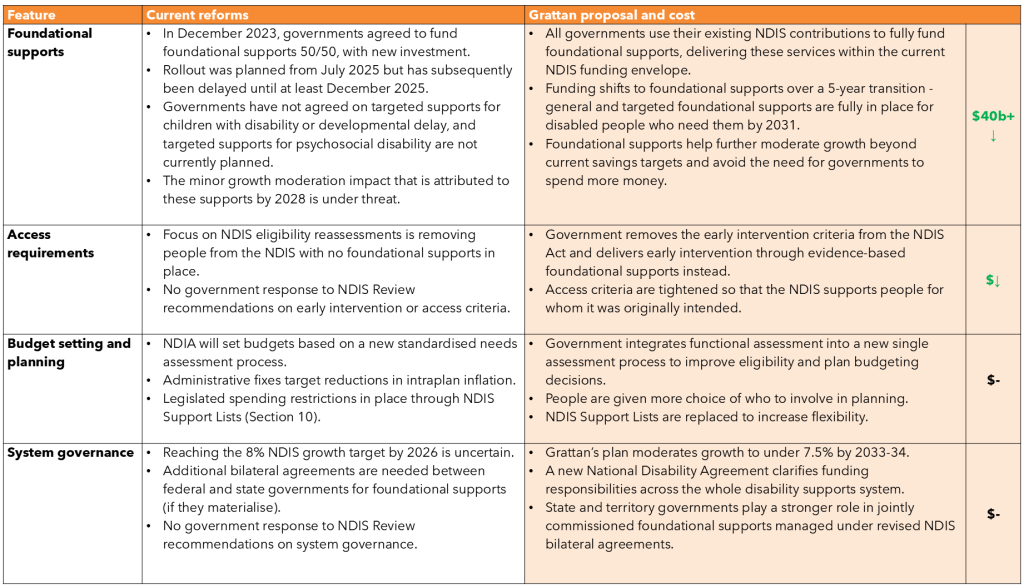
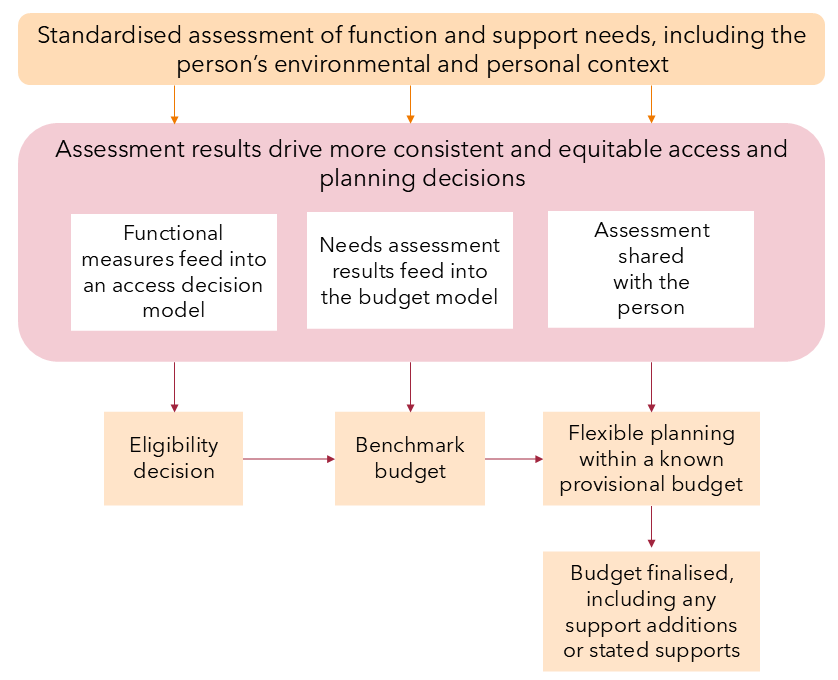
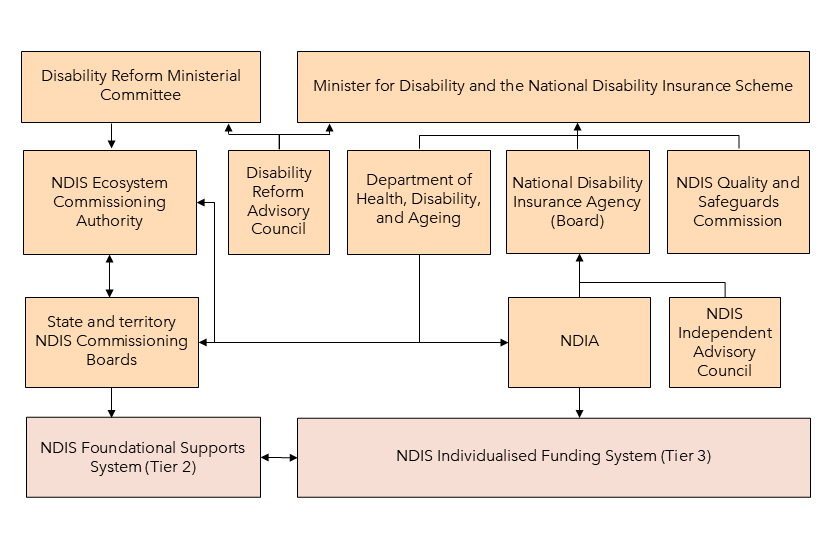
Figure 1: Grattan Institute’s proposal to rebalance the disability services system and deliver better results
The National Disability Insurance Scheme (NDIS) provides life-changing support to hundreds of thousands of Australians with significant and permanent disability. But not all people with disability are well served by the scheme, and many miss out altogether. At the same time, the costs of the NDIS have risen far higher and faster than expected, putting pressure on government budgets.
The NDIS cost $41.8 billion in 2023-24, making it one of the fastest growing areas of federal spending. Design flaws and governance failures baked in from the start have persisted. As spending on the NDIS has grown, other disability services have contracted, limiting support options for people outside the scheme.
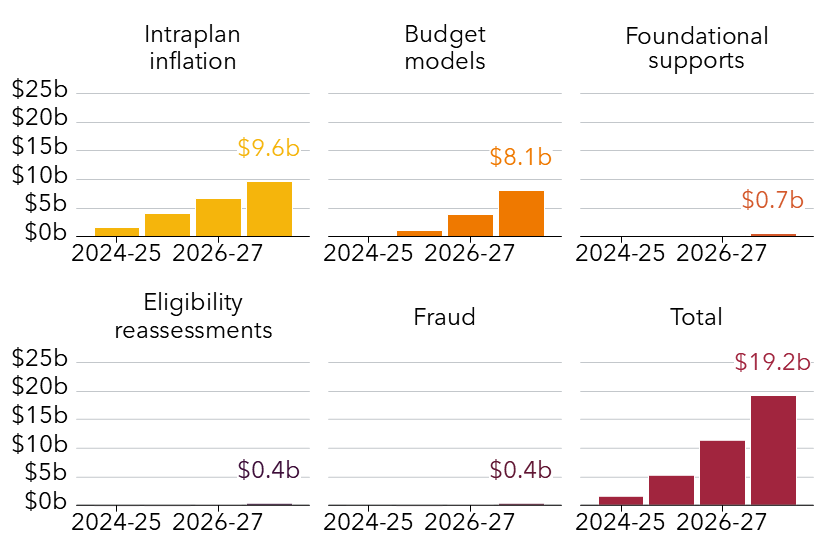
Governments have begun to act. Legislative and operational reforms initiated by the Albanese government in its first term aim to reduce cost growth to 8 per cent a year, in line with the 2023 National Cabinet agreement. If successful, these measures could save more than $19 billion over the next four years.
But there is no guarantee these reforms will succeed, and the current scope of measures is inadequate to deliver the scale of change needed. Even 8 per cent annual growth is untenable in the long term, far exceeding growth in other comparable government programs.
To put the NDIS on a stronger footing, governments need to follow through on current reforms and go further. A more balanced system – with clearer boundaries, fairer plans, and broader support options beyond individualised funding – is essential to ensure the NDIS delivers effectively and remains affordable into the future.
1.1 The NDIS costs a lot and continues to grow
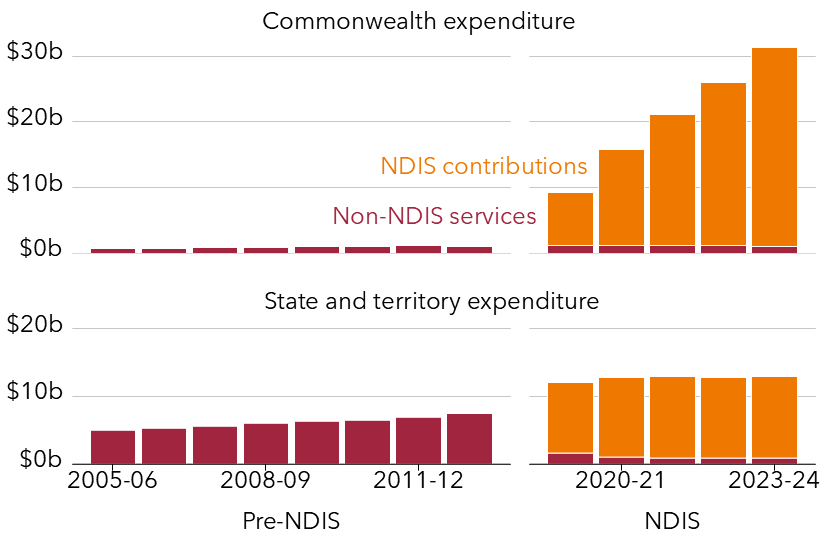
Before the NDIS was established in 2013, Australia lagged behind many comparable countries in the amount of money spent on disability. The same cannot be said today.1Grattan Institute analysis of Eurostat social protection data (European Union (2024)) and Productivity Commission Return on Government Services data(Productivity Commission (2024)).
The federal government and the states and territories are spending more than ever before on disability. Overwhelmingly, this expenditure is made up of their respective contributions to the NDIS (see Figure 1.1).2Ibid.
The federal government is responsible for an increasing share of the total, as a consequence of bilateral agreements which capped state contributions and saddled the federal government with the upside growth risk.3NDIA (2022a). Even so, total state and territory disability spending also rose from about $7.4 billion in 2013 – before the NDIS was introduced – to more than $12 billion by the end of the NDIS transition in 2020.4The 2013 figure is from Productivity Commission (2016) and the 2020 figure is from Productivity Commission (2025). The 2013 figure is inflated to 2023-24 dollars using the General Government Final Consumption Expenditure (GGFCE) chain price deflator.
NDIS expenses are estimated to be 1.7 per cent of Gross Domestic Product (GDP) in 2024-25, rising to 2.1 per cent by 2033-34.5NDIA (2024a, p. 7). The NDIS is now one of the fastest growing areas of federal government spending.6Commonwealth of Australia (2023, pp. xiv–xv).
The 2023 Intergenerational Report projected that spending on the NDIS could rise to as high as 6.3 per cent of GDP by 2062 if there were no moderating effect on growth from NDIS reform, which is higher than the projection for health spending over the same timeframe.7Ibid (pp. 157–158).
It is disappointing that discussions about NDIS sustainability are disproportionately focused on the costs side of the ledger. Costs of the scheme are much clearer and simpler to pin down than its benefits. The NDIS is undoubtedly providing wellbeing and economic benefits to the people it supports, their families, and the wider community, but meaningful cost-benefit analysis is impeded by current data limitations and a lack of effective measurement.8NDIS Review (2023a, p. 1155), and Miller et al (2023, pp. 14–17).
While this situation clearly must improve to enable more balanced analyses, from a purely fiscal perspective the level of growth of the NDIS greatly outstrips other comparable areas of spending and will not be sustainable on an ongoing basis in the context of competing pressures across all functions of government.
1.1.1 How the NDIS compares to other government programs
The NDIS was the third-largest expense program in the federal budget in 2024, with only support to seniors and revenue assistance to the states and territories costing more.9Commonwealth of Australia (2025a, p. 119).
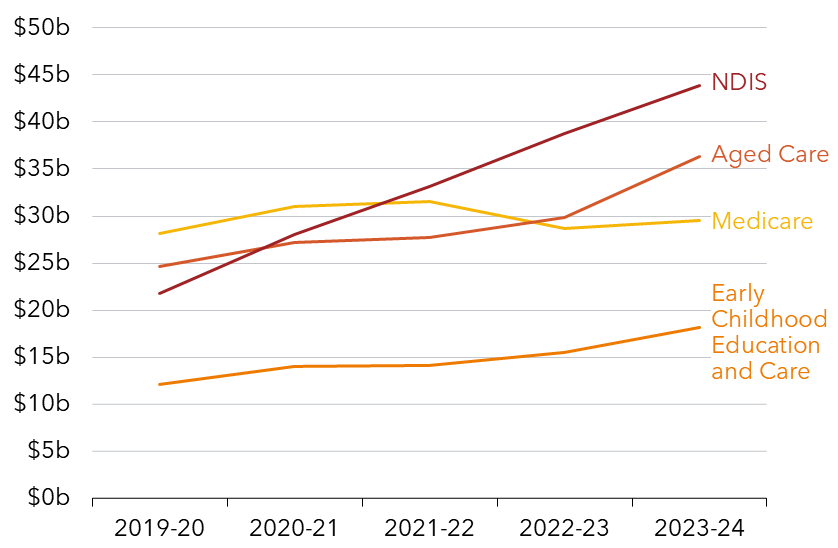
NDIS expenses are expected to grow to more than $58 billion by 2028, and that’s assuming the targets set by National Cabinet in 2023 are hit and annual growth moderates from about 24 per cent on average per annum from 2019-20 to 2023-24 to 8 per cent.10See NDIA (2024a, p. 8), and Grattan analysis of NDIA data from NDIA (2024b, p. 62).
Compared to other large social expenditure programs, an annual growth rate of 8 per cent is still high (see Figure 1.2). Aged care payments are projected to grow by 5.2 per cent from 2024-25 to 2025-26, while Medicare is projected to grow by 5.6 per cent.11Commonwealth of Australia (2025a, p. 75).
Figure 1.1: Australian governments are spending much more on disability services than they were before the NDIS
Expenditure on direct disability service delivery, 2023-24 dollars
Note: Includes all expenditure on direct disability service delivery by Australian governments. Sources: Productivity Commission (2025) and Productivity Commission (2016).
1.2 More people are in the NDIS than it was designed for
The sheer number of people in the NDIS is a significant source of cost growth.
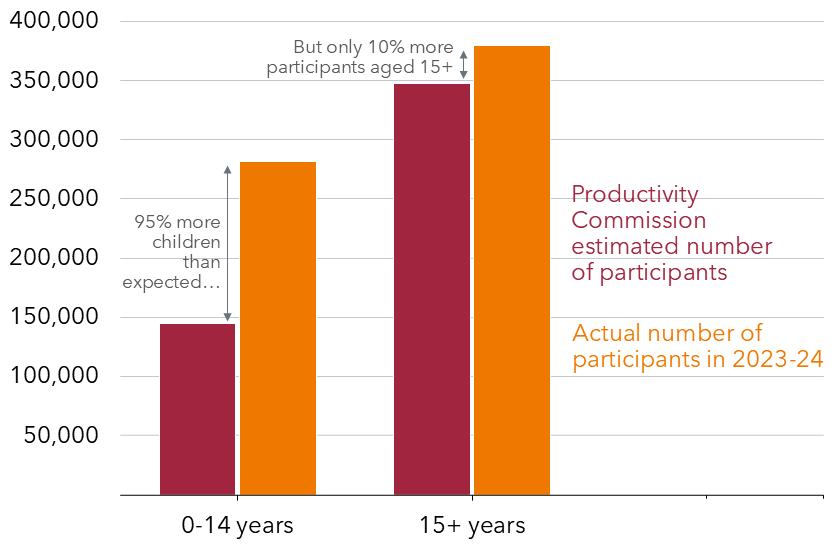
In 2011, when the Productivity Commission initially proposed the NDIS for people with lifelong and severe disability, it estimated the scheme would reach 490,000 people, accounting for population growth.12Productivity Commission projection (Productivity Commission 2011), inflated by Grattan Institute to account for population growth using ABS Estimated Resident Population: (ABS (2024a)). In fact, it now supports more than 700,000 people and this is projected to surpass a million by 2034.13NDIA (2025a, p. 17), and NDIA (2024a, p. 78). The number of adults is only a little higher than originally expected; the number of children, however, is nearly double (see Figure 1.3).
The number of disabled people entering the NDIS was expected to stabilise from 2020 after the initial transition period when people already getting support from state and territory programs moved across into the national scheme.
This has happened for most groups, with the significant exception of children with developmental delay or autism, who now make up almost half (44 per cent) of all people on the NDIS.14NDIA (2024c, p. 28), and Grattan analysis of NDIA (2025b, Table 8) and NDIA (2025a, p. 101). About 11 per cent of all Australian six-year-olds were on the NDIS in March 2025, including 15 per cent of six-year-old boys.15NDIA (2025a, p. 18).
Figure 1.2: NDIS spending is growing much faster than other government social care spending
Government expenditure, 2023-24 dollars
Note: Dollar amounts inflated to 2023-24 dollars using the General Government Final Consumption Expenditure chain price deflator (see Productivity Commission (2025)). Sources: Productivity Commission (2025), NDIA (2024b), and Department of Health, Disability, and Ageing (2024a).
A growing number of people with chronic health conditions are also turning to the NDIS for support. NDIS data at the end of 2022 showed there were more than 41,000 people on the scheme with a chronic health condition listed as their primary disability.16NDIS Review (2023a, p. 73). This is despite people with chronic health conditions being explicitly excluded from original modeling of NDIS costs as not being among the intended beneficiaries of the scheme.17Productivity Commission (2011, Appendix H).
While numbers of new entrants for all major disability types fell below what was expected last year, it appears likely this resulted from operational challenges rather than any genuine decrease in demand.18NDIA (2024a, pp. 50–52).
Accordingly, new entrants are expected to increase again from 202425, as the National Disability Insurance Agency (NDIA) ‘catches up’ on its backlog of eligibility assessments.19Ibid (p. 16).
1.2.1 People don’t leave the NDIS once they have joined
Not only are there many more people in the NDIS than it was designed for, people tend to stay in the scheme for the long term, putting more pressure on its sustainability.
People leave the scheme either because they pass away, because they leave voluntarily, or because they no longer meet the eligibility criteria. However, non-mortality exit rates have been consistently lower than expected.20Ibid (pp. 56–57). This is especially true for children, but also for over-65s, who make up a small but growing proportion of participants.
Most children stay in the scheme for the long term, even though the expectation was that many of them would receive early intervention for a fixed duration.21Productivity Commission (2011, p. 171). A greater focus in 2024 on reassessments to determine ongoing eligibility resulted in only half as many people leaving the scheme as was expected.22NDIA (2024a, p. 57).
Figure 1.3: There are far more children in the scheme than originally expected
Number of projected and actual participants by age bracket, 2023-24
Note: Productivity Commission estimates have been inflated based on population growth for 0-64 year-olds between the reference year (2009) and 2024, using Australian Bureau of Statistics Estimated Resident Population data. Sources: Productivity Commission (2011), NDIA (2024d), and ABS (2024a).
This means that some people joining as infants could stay in the NDIS until they are 65 years old or longer. Even with less expensive plans, this could add up to $1.7 million in average lifetime expenditure per person in the NDIS.23Ibid (p. 102). A sustainable scheme must ensure that the benefits to people with disability – and to taxpayers – of remaining in the NDIS are greater than or equal to the cost.
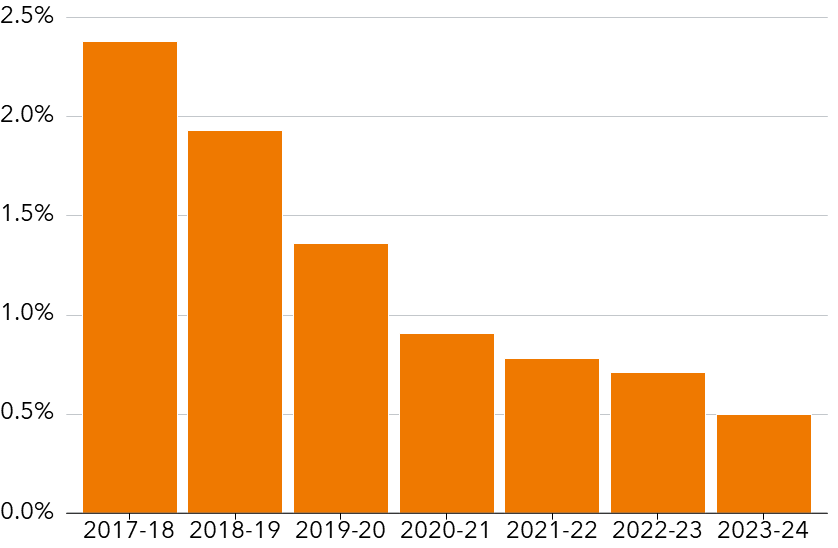
Over-65s are putting increasing pressure on NDIS sustainability
As at March 2025, there were more than 37,000 people on the NDIS over the age of 65.24NDIA (2025a, p. 99). This is a growing proportion of all people on the NDIS, rising from 2.4 per cent in 2019 to 5 per cent in June 2024, at a total cost of $3.7 billion.25Grattan analysis of NDIA (2019a, p. 81), NDIA (2024b, p. 82), and NDIA (2024e). This group is projected to grow to 7.6 per cent of people on the scheme (78,151 people) by 2034.26NDIA (2024a, p. 71).
While it is possible for someone to choose to transfer from the NDIS to aged care when they reach 65, in practice this rarely occurs because of the higher per-person funding available on the NDIS versus aged care, and the absence of means testing in the NDIS.27NDIS Review (2023a, p. 181).
Over-65s tend to have high-cost plans, with the median at about $93,000 per person per year.28This figure is the average annualised budget at the 50th percentile: Unpublished NDIA data, 2025. This group will continue to grow as a proportion of people on the NDIS in the years ahead. Without significant changes in aged care policy settings, it is unlikely the current trend of seniors staying on the NDIS will change.
1.2.2 There is nowhere else for people with disability to go
One of the reasons the NDIS has attracted so many entrants is that there are very few disability services available for people outside the scheme.
Funding for disability services is concentrated in the NDIS; and yet, there are many thousands of Australians who might benefit from some level of support who aren’t eligible.29For example, the 2023 NDIS Review illustrated the insufficiency of Home and Community Care services for people under 65 not eligible for the NDIS, including people who had lost access to these supports when they were moved into the new scheme: NDIS Review (2023a, p. 76).
At the inception of the NDIS, the states and territories included significant in-kind contributions to meet their funding commitments by rolling their existing services into the new scheme.30NDIA (2022a). They also discontinued many established services where it was assumed, rightly or wrongly, that the NDIS would pick up the slack. Services deemed ‘ILC-like’ (that is, providing information, linkages, and referrals) were transitioned into the NDIS,31Productivity Commission (2017, p. 30). while others were allowed to wither as contracts ended.
The scale of the drawback of non-NDIS disability services varies across the states and territories.32Grattan Insitute analysis of Productivity Commission (2024). But the overwhelming picture is of thin to non-existent coverage for people with disability who are ineligible for NDIS support.33Recent research found that 90 per cent of surveyed disabled people without support from the NDIS said that the support and services they rely on in their day-to-day lives are inadequate to meet their needs: Olney et al (2022, p. 13).
Compounding this issue, there is little evidence that the promises made in successive federal government and state/territory disability strategies of more accessible and inclusive mainstream services for all disabled people have materialised.34The 2025 progress report on Australia’s Disability Strategy 2021-31 showed either no change or regress in 29 of 43 measures: AIHW (2025a, p. xi). Quite the opposite: as costs have been shifted to the NDIS from health, education, justice, and housing, the states and territories have sought to minimise their funding responsibilities.
To make matters worse, there is no overarching agreement or mechanism proposed to clarify funding and implementation responsibilities and promote cooperation and accountability across federal, state, and territory governments.35Productivity Commission (2019, p. 5). The current National Disability Agreement was crafted in 2008, long before the NDIS even existed.36Ibid (p. 70).
As it stands, disability services in Australia have become an all-or-nothing proposition: either you get an NDIS plan, or you get minimal mainstream services.
Foundational supports are essential to NDIS sustainability, but are yet to be implemented after a decade
In a world where disability insurance begins and ends with the NDIS, there is a strong incentive for the more than 2 million disabled Australians under 65 to join the scheme, and a strong disincentive for anyone to transition out of it. The results are increased dependence on individualised funding, and rising costs.
‘Foundational supports’ is the new name the 2023 NDIS Review gave to lower-level disability supports not delivered as individualised funding (See Box 1).37NDIS Review (2023b). These supports are integral to the vision of bridging the gap between individually funded NDIS supports that are available to some, and mainstream and community services that are available to all.38Productivity Commission (2011).
These supports were part of the original design for the NDIS and were intended to help prevent, reduce, or delay the need for people to get specialist disability services, by improving their access to community and mainstream services and building their capacity to participate in the community and economy.39Council of Australian Governments Disability Reform Council (2015a, pp. 1–4). But these supports are mostly absent in Australia today.
While foundational supports are beginning to be built back up in less fiscally challenged jurisdictions, notably WA,40WA’s Department of Communities is establishing a Communities Inclusion Connection Team to facilitate connections to community and mainstream services, with a focus on ‘family-led, place-based, community supports that will increase equality of opportunity and access to early intervention and foundational supports for people with disability’: Western Australian Department of Communities (2024). there remains considerable distance between today’s singular focus on individualised NDIS funding and the more balanced configuration of disability services and supports that Australia needs.
Building up foundational supports can help to change these incentives, and stem the tide of people turning to the NDIS as the sole source of support. Commissioning a broad range of foundational supports would mean there is a viable substitute for individualised funding, ensuring many disabled people are well-supported in a more cost-effective way.
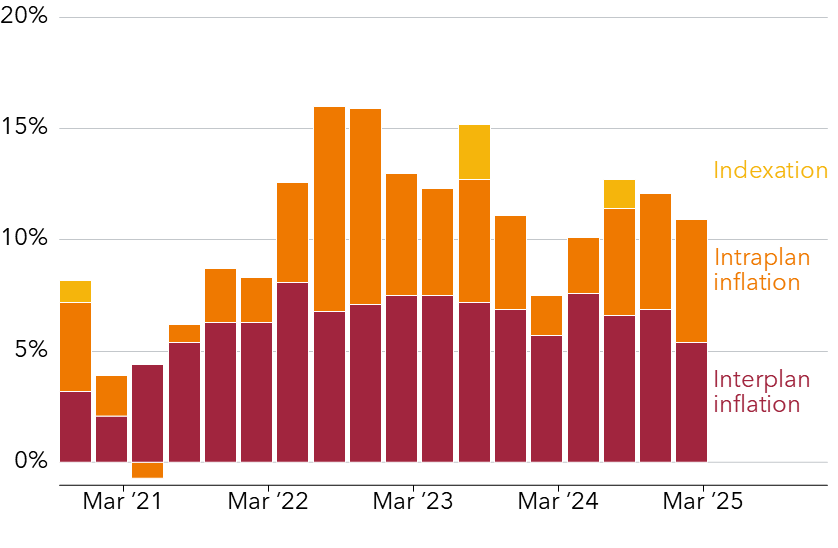
1.3 People’s plans grow well above inflation on average
Not only is the number of people in the NDIS large and growing, how much funding each person gets tends to increase year on year as well.
Box 1: What are foundational supports?
Foundational supports are services and supports for people with disability that do not involve individualised funding from the NDIS. Foundational supports are specifically for disabled people and their families – they are not the mainstream services that everyone, including people with disability, also uses.aThe exact design of foundational supports is subject to government negotiations.
There are two streams of foundational supports: general and targeted.
General foundational supports are for all people with disability. They include services such as: ∙ information about disabilities; ∙ help in developing self-advocacy and supported decision making; ∙ peer support programs; ∙ educational and parenting programs for parents and carers of people with disability; ∙ social and community activities; and ∙ information about local mainstream services, and referral to other forms of support.
Targeted foundational supports are supports that are aimed at particular groups of disabled people. Many are early intervention supports and services for disabled people with specific needs who are not eligible for individualised funding from the NDIS. They sit between this funding and general foundational supports in terms of intensity. Targeted foundational supports include: ∙ programs and supports for children and their families that build their independence and social skills; ∙ low-to-mid-level allied health supports to improve the long-term capabilities of children; and ∙ early intervention programs and services for people with psychosocial disability.
Foundational supports will be funded as commissioned services, meaning that organisations and providers will be contracted to deliver a new set of programs or supports. Foundational supports are not funded through individualised packages, unlike other supports in the NDIS.
Anyone with a disability and their families can access general foundational supports, including people who are in the NDIS or who are also receiving targeted foundational supports. However, people who are in the NDIS cannot access targeted foundational supports, and people accessing targeted foundational supports cannot simultaneously access the NDIS.
The growth in average payments per person on the NDIS was 7 per cent over 2023-24.41NDIA (2024a, p. 62). Payments increase for many reasons, including inflation, changes to enterprise bargaining agreements, or people becoming eligible for more intensive supports.42Ibid (p. 62).
However, there is a persistent trend in people receiving more money with each new plan, that can’t be completely explained by these reasons. A significant contributing factor is likely to be the unstable and continually changing practical interpretation of what is deemed reasonable and necessary by each planner.43NDIS Review (2023a, p. 249).
The upshot of higher numbers entering the NDIS and persistent growth in payments is that overall NDIS costs have grown by an average of about 24 per cent per year over the four years to 2024. Even though growth has slowed to 10.6 per cent in the third quarter of 2024-25, getting this down to 8 per cent by 2026 will be challenging.44NDIA (2025a, p. 7).
1.3.1 The need for intensive support is rising
Nearly 40 per cent of the cost of the NDIS goes to about 7 per cent of people with the most intensive support needs.45These figures are for total plan size, not only the Supported Independent Living component: Bennett and Orban (2024a). Such supports include housing and intensive in-home support for people with the most profound disabilities.
The number of people transitioning to intensive funding is projected to further increase steadily as more parents from the Baby Boomer generation grow too old to care for their disabled children, and people age within the scheme.
The number of people receiving intensive funding is projected to grow to more than 50,000 by 2033, compared to about 36,000 today.46Ibid (p. 12). With average payments exceeding $430,000 per person per year, this represents a major cost pressure.47NDIA (2025a, p. 67).
There has been little innovation in how these services operate since the inception of the NDIS, with service models largely unchanged.48NDIS Review (2023a, p. 591). A previous Grattan Institute report explained how government should introduce more innovative and cost-effective housing and living supports for people with profound disability.49Bennett and Orban (2024a). But the absence of better, safer, and more sustainable alternatives persists.
1.3.2 The NDIS doesn’t operate like an insurance scheme
The original NDIS design was for a multi-tiered scheme with different levels of coverage, clear and enforceable eligibility criteria, data-led resource allocation, and a sophisticated operational risk-management approach.50Productivity Commission (2011). In short, a robust insurance model to manage life-long disability support needs and costs.
The current NDIS has none of these things in place as it continues to grow, and the NDIA has insufficient policy levers to help manage mounting pressures.
The NDIS needs to develop these policy levers if it is to stand a chance of stopping cost blow-outs and becoming sustainable.
For example, the way the NDIS system has created plans and apportioned funding to date helps to explain why average payments keep increasing.
An insurance approach would equitably distribute funding based on the estimated needs of people in the NDIS, with a clear link between individual plans and overall resources.
But in practice, the task of deciding each person’s NDIS supports has been left in the hands of well-meaning, junior bureaucrats working with vague and complex criteria through a process that is disconnected from the total budget.
Inconsistency and inequity is hard-wired into the NDIS design. This has made it hard to control costs. It has also served disabled people very poorly, because the system invites disputes and uncertainty over future funding for supports.
Legislative changes last year have set a path for rectifying this issue through a new standardised assessment and planning framework, which will replace the current model once designed and set out in rules. But getting this new process established is technically complex, requires extensive engagement with disabled people, and won’t happen overnight.
1.4 The problems in the NDIS are long-standing
With a lack of disability services outside the NDIS, a low bar to entry, and a lack of effective claims management in the scheme,51We refer to claims management throughout the report as a principle of insurance systems, rather than the specific process of paying for supports in the NDIS which is sometimes referred to as ‘claims’ or ‘claiming.’ it is unsurprising that the NDIS is fast becoming unsustainable as more and more people join and plans increase above inflation year on year.
The issues that now threaten the NDIS are the result of long-standing failures in scheme design and governance that have come into increasingly stark relief as the program has grown in size and cost.
Since the early years of the NDIS transition, there have been more entrants than expected in key population groups, not enough people leaving the scheme, plan budgets and plan inflation consistently higher than expected, and concerns about inconsistent and inequitable decision-making.52See the 2015-16 Annual Financial Sustainability Report: NDIA (2016a).
When these issues were initially reported in 2016, the NDIS was supporting only 30,000 people across nine trial sites at a total cost of $2.4 billion.53NDIA (2016b, pp. 27, 57). Fast forward to 2025 and it is only the size of the scheme that has changed, not the issues it faces.
In the intervening nine years, successive governments have been enthusiastic in conducting reviews of the scheme, which have consistently identified many of these same pressures and made recommendations to address them.54Ernst & Young (2015), Productivity Commission (2017), Tune (2019), and NDIS Review (2023b).
What has been missing up to now has been the urgency and commitment to see through the fundamental reforms needed to put the NDIS on a sustainable footing.
The current burning platform of NDIS sustainability, and the potential for well-conceived reforms to move the dial on service quality and results as well as cost growth, presents a unique improvement opportunity that governments and the disability community cannot afford to miss.
1.4.1 Beware of hitting the target but missing the point
The 8 per cent growth target for the NDIS set by National Cabinet in 2023 has been a critical focusing mechanism for government effort over the past 18 months.
It helped pave the way for legislative changes that should simplify the administration of the NDIS. Those changes provide some useful tools to moderate growth, including through introducing time intervals for plan spending, and better facilitating the eligibility reassessment process.55Parliament of Australia (2024).
More important in the long term, the changes pave the way to more predictable and consistent budget setting processes, as described in Section 1.3.2.
Significant savings totaling more than $19 billion have been attributed to these and other measures which are baked into the forward estimates for the NDIS, but it is too early to say with confidence that these savings will be realised.56NDIA (2024a).
While there is some indication that the growth rate has begun to moderate over recent quarters, with 10.6 per cent growth projected for 2024-25,57NDIA (2025a, p. 7). this cannot solely or confidently be attributed to the impacts of reform.
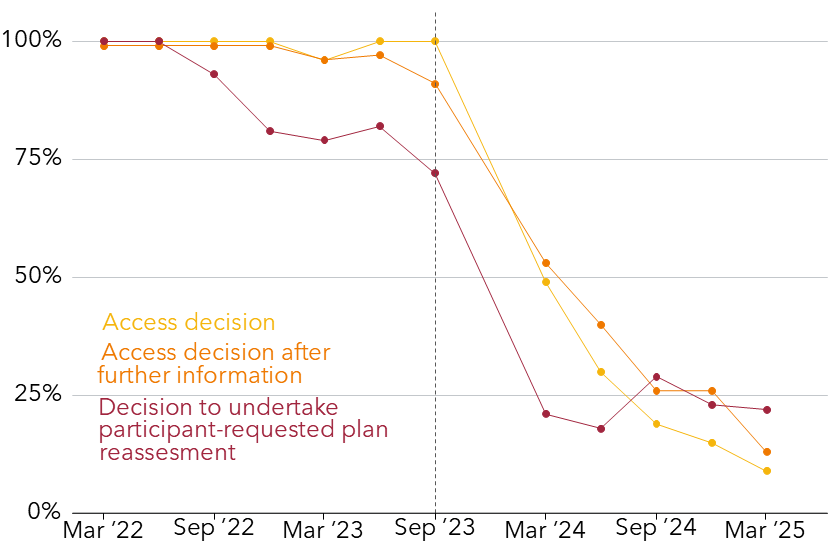
A significant downturn in operational performance is very likely a contributing factor. The NDIS is groaning under the weight of unsustainable work volumes, with about 91 per cent of new applicants waiting more than the ‘guaranteed’ 21 days for an access decision, and 78 per cent of people who request a reassessment getting no response within the same guaranteed time-frame (see Figure 1.4).58Ibid (p. 109).
It will be important that growth moderation is achieved through measures that do not result in vital supports being delayed or disabled peoples’ experience and prospects of meaningful results from the NDIS being undermined.
Figure 1.4: Operational performance has tanked since September 2023
Proportion of cases meeting the Participant Service Guarantee timeframe in each quarter
Notes: ‘Access decision’ refers to metric two: ‘Make an access decision, or request for more information, after an access request has been received’. ‘Access decision after further information’ refers to metric four: ‘Make an access decision, after more information has been provided’. ‘Decision to undertake participant-requested plan reassessment’ refers to metric 12: ‘Decide whether to undertake a Participant Requested Plan Reassessment, after the request is received’. Data is unavailable for December 2023 due to the NDIA upgrading to a new computer system. Sources: NDIA (2024c), NDIA (2024b), NDIA (2023a), NDIA (2023b), NDIA (2022b), NDIA (2022c), and NDIA (2025a).
This will remain a risk even as current reform measures begin to bear fruit, since the current package of reforms does not address the full gamut of changes needed to ensure the NDIS really delivers for disabled Australians.
Growth moderation is a necessary goal, but it should not mean that the people who need support from the NDIS get sub-optimal results.
Without further bold policy decisions, government risks hitting the target but missing the point.
Fraud and rorts are only a small part of the story
So far, the federal government has focused heavily on waste and fraud, without using all of the policy levers that are likely to help control costs, including adjusting eligibility criteria, establishing foundational supports, and reforming NDIS planning processes.
While combating fraud is vitally important for the integrity of the NDIS and to ensure that funding and quality support gets to the people that need it, it is not a major contributor to meeting current savings targets. The expected savings from fraud and compliance initiatives over the next three financial years total $424 million, just over 2 per cent of current projected savings and less than 0.3 per cent of total projected scheme expenses over the period.59See Parliament of Australia (2025, p. 48). The federal government invested $168.1 in 2025 for the Crack Down on Fraud program and improving the NDIA’s ability to detect and respond to fraud and non-compliant payments (Commonwealth of Australia (2025b, p. 73). This follows investment of $194.3 million in 2024 to better detect and prevent fraud (Commonwealth of Australia (2024a, p. 172) and Commonwealth of Australia (2024b, p. 295)), and $126.3 million in 2022 to establish the cross-agency Fraud Fusion Taskforce (Commonwealth of Australia (2022, p. 9)). As of December 2024, there was only $35.9 million of fraud under investigation (NDIA (2024c, p. 101)).
1.5 The NDIS is worth saving
Before the NDIS, people with disability described their lives first as shut in institutions, and then as shut out of Australia’s society and economy; as isolated, marginalised, and lonely; as a struggle for resources that were persistently uncertain.60National People with Disabilities and Carer Council (2009), and Productivity Commission (2011).
Disability services were minimal and frequently crisis-driven. They were often restricted to people with the most severe disability, with many others missing out altogether.61Productivity Commission (2011, pp. 5–7). Services were block-funded by state and territory governments at a quarter of what the NDIS funds today, and changed with government budget cycles, leaving people uncertain about what would be available to them in the long term.62Based on the Productivity Commission’s estimate that state and territory funding of disability services totalled about $8 billion (Productivity Commission (ibid)), which, inflated to 2023-24 dollars, is about $11.2 billion, or 27 per cent of total NDIS payments in 2023-24 of $41.8 billion (NDIA (2024b)).
The costs of lifelong and severe disability are immense. And Australians with disability tend to earn less than non-disabled Australians on average, with 45 per cent of people with disability in the bottom 40 per cent of equivalised gross household income, making it even harder to afford disability services.63This compares to 25 per cent of people without disability in the bottom 40 per cent of equivalised gross household income. See ABS (2024b).
The NDIS is a bold and ambitious solution to the inequity and costs that people with disability face, and one that disabled people fought for over decades. Instead of a heavily rationed discretionary program, the NDIS is a rights-based scheme that provides a funding entitlement which ensures that if you have or acquire a lifelong and severe disability and are under the age of 65, you are covered.
The NDIS has transformed the experience of disability in Australia. People who need mobility equipment can get it, where previously it may have been unaffordable. Adults with intellectual disability who have had few options other than to continue living with aging parents have the opportunity to live independently. Families who worry about how they will support their disabled relatives have peace of mind that the NDIS is there to meet their needs.
Many people with disability and their families benefit from the NDIS, reporting major improvements in their daily living, relationships, health, well-being, social and civic participation, and choice and control.64NDIA (2024f, p. 16).
And yet, the NDIS is under threat from spiraling costs, with indications that the social contract on which it depends is beginning to fray. The NDIS today has significant problems that governments must address to make the scheme sustainable.
The NDIS is worth saving. Getting necessary reforms embedded is achievable during the current term of federal government, needn’t mean spending more overall, and will yield benefits for our economy, our prosperity, and our diverse society.
1.5.1 What this report does not do
This report focuses on the structure of the NDIS and demand-side issues such as managing claims in a social insurance program.
There are other avenues that could potentially make the NDIS more sustainable that are out of scope for this report, including tax reforms to raise more revenue and lower the amount of interest the government has to pay for borrowings to fund the NDIS, and supply side issues, such as workforce productivity which could reduce the amount of money government needs to spend per person over time. These are important areas for future research.
1.5.2 This report explains how government can save the NDIS
This report explains how government can make the NDIS sustainable and create a better experience for people with disability and their families, all without spending more money.
This involves major reforms to the NDIS. Some of these reforms require staying the course with existing measures, while others are entirely new or represent a change to current reforms.
This includes making substantive progress in establishing a whole new system of disability services – foundational supports. The recent co-location of disability with health and aged care at ministerial and departmental level provides a new and unique opportunity to ensure these supports integrate well with existing service systems.65Commonwealth of Australia (2025c, pp. 20–22).
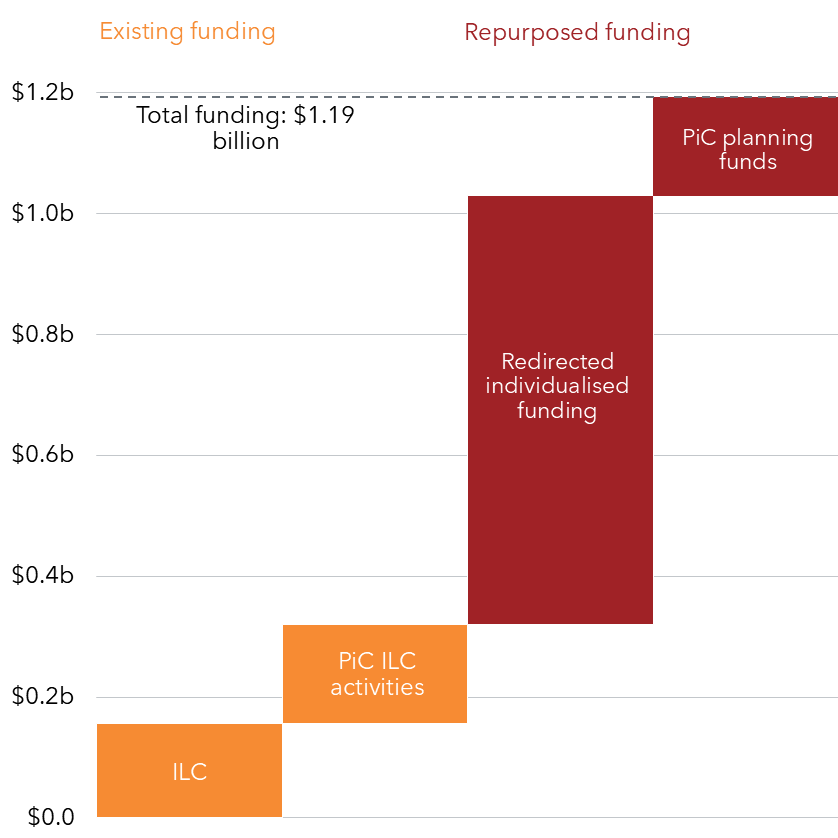
An accurate picture of the costs to government of getting the NDIS back on track under its current plans should include funding for these foundational supports. Grattan Institute conservatively estimates that foundational supports would need $6.4 billion per year once fully introduced.
Yet the pathway to this outcome is highly uncertain. The prospect that state governments will find significant new money to fund these services while managing other fiscal pressures remains distant.
It is unlikely that foundational supports will materialise in any meaningful way during the current term of federal government without new and different thinking.
The current impasse in Commonwealth-state negotiations could be overcome by governments agreeing to re-purpose a portion of the combined NDIS contributions they have already committed.
By setting a ceiling for individualised funding, managing the scheme’s liabilities more effectively, and redirecting committed NDIS funds to establishing a sufficient range of alternative supports and services, we argue in this report that foundational supports can be fully funded within the existing budget estimates in a way that further moderates scheme growth beyond current committed savings targets. Our plan would deliver three major improvements:
A reduction in projected NDIS payments of about $12 billion over the next 10 years, and a further saving of $34 billion over the same period from not requiring new money to fund foundational supports.66These savings and all costings in this report are calculated based on an adjusted version of the June 2024 Annual Financial Sustainability Report projections. For information about the costing methodology, see Appendix A.
A more targeted focus for individualised funding and an improved experience for people with the most significant disabilities, who need the NDIS for their lifetime.
A wider net of disability insurance that ensures more disabled people can get the help they need in the most efficient and effective way through a range of nationally underwritten, and locally responsive foundational supports.
IN THIS CHAPTER
Share
2 Better boundaries around the NDIS
The NDIS was designed to provide long-term support to Australians under 65 with significant and permanent disability. By pooling the risk of disability across the population, it aims to provide disabled Australians with choice of supports to help them live independently and participate in society.
But the NDIS has not been able to function fully as an insurance scheme. Its eligibility criteria, together with policy settings that use lists of diagnoses to shortcut decision making, have made it difficult for the National Disability Insurance Agency to manage access and costs effectively. Many more people have entered the scheme than was originally expected.
To make matters worse, the evaporation of services outside the NDIS has put pressure on the scheme and made it vulnerable to cost-shifting from other service systems.
To remain sustainable, the NDIS needs clearer boundaries to define who is eligible and what kinds of support the scheme is responsible for.
This chapter explains how government should tighten eligibility criteria while ensuring that disabled people who don’t need individualised NDIS funding can still get essential support through a strengthened system of foundational supports.
2.1 The NDIS is designed for people under the age of 65 with lifelong and severe disability
Before the NDIS, disability services in Australia were fragmented, unfair, inefficient, and uncertain. People with disability and their families had no guarantees that they would get support, or at the level they needed, or for as long as they needed.67Productivity Commission (2011).
People with disability tend to be much poorer than people without disability. One Australian study found that adults with disability need to increase their disposable income by 50 per cent to enjoy a similar standard of living as adults without disability.68Vu et al (2020).
People with disability in Australia face social marginalisation and rejection, discrimination, poorer health, unnecessarily shortened life expectancies, and countless other limitations.69Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (2023), ABS (2024b), and Trollor et al (2017).
In short, the costs of severe, lifelong disability are immense.
Most people and families cannot prepare for the costs of significant disability.70Productivity Commission (2011, pp. 114–116). Because almost nobody could save enough to cover themselves against the risk of severe, lifelong disability, and given the absence of an accessible private disability insurance market, it makes sense for the government to pool the risk across the population and provide this much-needed insurance for Australians.
Disability also increases with age (see Figure 2.1).71ABS (2024b). However, age-related disability is something that people can plan for by saving for their retirement and aged care needs. And people receive help with these costs from the government through the aged-care system. Having a severe disability during income-earning years is a very different risk – much less likely, and much more consequential – and therefore needs a different insurance approach.
Short-term or less-severe disability also brings extra costs to people compared to their non-disabled peers.72Vu et al (2020). However, these costs tend to be smaller and less disruptive to people’s lifetime earnings and social participation, compared to people with severe disability.
While there need to be services and supports available to people with shorter-term or less-severe disability, their impact means that people need much less insurance and protections than is guaranteed by the NDIS.
The NDIS is a rights-based scheme that covers people against the impoverishing costs of severe disability. But it has also stimulated a market of services and supports that far outstrips what was available previously.
An unsustainable NDIS risks upending this essential coverage for Australians with permanent and profound disability.
2.2 Eligibility criteria should set clear boundaries around the NDIS
Eligibility criteria are a key tool for managing the high demand for NDIS services and funding. They serve as a ‘frontline protection’ against the scheme expanding beyond its intended scope, and they help guard against cost-shifting from other government sectors such as health, housing, and education.73Walsh and Johnson (2013).
The Applied Principles and Tables of Support (APTOS) were intended to govern the overlap between the NDIS and other service systems.74Council of Australian Governments Disability Reform Council (2015b). However, APTOS has had limited impact on eligibility decisions because it primarily relates to what supports someone can access and is subordinate to the NDIS Act and Rules.75NDIS Review (2023a, p. 135).
Unlike previous programs, the NDIS is demand driven and does not have a budget cap, meaning anyone with a lifelong, severe disability can get support. While this is crucial for providing coverage to those who need it and are entitled to it, it also means the NDIS must manage the risk of very high demand, which could become unaffordable for governments and taxpayers.76Sturgess (2013).
Figure 2.1: Disability increases with age
Proportion of Australians with disability, by age and sex, 2022
Source: ABS (2024b).
To make the NDIS sustainable, it is essential to manage claims through effective eligibility criteria. Clearer and firmer boundaries are needed to ensure the scheme remains financially viable.
2.2.1 Current criteria are vague and complex to administer
There are two access routes to the NDIS: you can enter with a lifelong need for disability supports through the disability requirements, or you can enter if you are likely to benefit from early intervention from the NDIS through the early intervention requirements.77A person would meet the early intervention requirements if they have an impairment that is likely to be permanent, are likely to benefit from early intervention supports, and the early intervention supports they need are NDIS supports (that is, they are funded by the NDIS). There are some variations for certain groups. See NDIA (2025c).
The NDIS was designed to be disability-type and diagnosis agnostic. For people under the age of 65 who meet residency requirements, access is based on whether their impairment is permanent (or likely to be) and whether it significantly limits their functional capacity.
This approach remains appropriate. It helps ensure people aren’t excluded based on diagnosis.
Access to the NDIS under early intervention requirements is based on whether receiving supports is likely to reduce pressure on informal supports, or help a person improve or maintain their function or build capacity.
But in practice, these criteria are hard to apply consistently.78NDIS Review (2023a, pp. 217–221). Key terms in the NDIS Act and Rules are poorly defined, leading to confusion and inconsistent decisions.79NDIS Review (2023a, pp. 229–238), and Tune (2019, pp. 71–77).
2.2.2 The NDIS admits people with a wide range of impairments
One consequence of this lack of clarity is that people can be granted access to the NDIS under the current criteria whose needs are not well suited to the intended purpose of disability insurance.
Chronic diseases are long-lasting health conditions with persistent effects that can reduce people’s quality of life. They are highly prevalent, often progressive, and frequently associated with lifestyle factors and aging.80AIHW (2024a). Common examples include arthritis, diabetes, heart disease, and cancers.
Chronic health conditions are typically treatable in their early stages and therefore don’t meet the NDIS’s permanence criteria. But when these conditions progress, treatment options may become limited and functional capacity may decline significantly – making NDIS access more likely. This occurs even though the Applied Principles and Tables of Support (APTOS) assign responsibility for early intervention and treatment of chronic conditions to federal, state, and territory health systems.81Council of Australian Governments Disability Reform Council (2015b, p. 3).
In 2022, there were more than 41,000 people in the NDIS with a chronic health condition listed as their primary disability, with a total liability of $2.46 billion, or 9 per cent of total scheme costs in that year.82NDIS Review (2023a, pp. 73–74).
Given the forecast increase in complex chronic disease in the Australian population at large, this cohort of people seems likely to grow as a proportion of people found eligible for the NDIS and as a share of scheme costs under the current access criteria.83Breadon et al (2022), and Department of Health, Disability, and Ageing (2022).
2.3 It is difficult to determine when some impairments are permanent
The application of the permanence criteria is straightforward in relation to many impairments that are obviously life-long, such as an intellectual disability or an acquired brain injury, and other impairments that are clearly time-limited, such as a temporary loss of mobility caused by a fracture from a fall.
But the application of these criteria is more difficult for people with psychosocial disabilities, because of their frequently episodic and fluctuating nature, and the lack of consensus among medical professionals and the community about when and if such impairments should be considered permanent.84Mellifont et al (2022, p. 271).
In consecutive reviews of the NDIS, health professionals report that people with psychosocial disability receive inconsistent eligibility decisions, even where they have similar psychosocial needs and circumstances.85Tune (2019, p. 73). This is reflected in patterns of access: since the NDIS began, people with a psychosocial disability applying to the scheme have been found eligible at far lower rates than people with other disabilities – 70 per cent versus an overall average of 85 per cent, as of June 2023.86AIHW (2024b, Table NDIS1).
Despite changes made to the NDIS Act in 2022 to clarify that psychosocial disabilities can be considered permanent even when they vary in intensity over time, eligibility rates for Australians with psychosocial disability have dropped even further in recent quarters – falling as low as 23 per cent in the third quarter of 2024-25.87NDIA (2025a, Supplement E, Table E5).
While the total number of people in the NDIS with a psychosocial disability today is broadly in line with the original estimates at around 65,000,88Productivity Commission (2017), and NDIA (2025a, Supplement E, Table E16). these persistent challenges mean it is hard to be confident that the people with psychosocial disability in the scheme today are the ‘right’ people, or that their episodic needs are well catered for and understood.
In practice, policing any entry line for this group is especially fraught, a challenge exacerbated by the high volume of unmet need for people who require some level of psychosocial support.89Health Policy Analysis (2024).
2.3.1 Permanence criteria are an increasingly porous boundary
The permanence criteria help to identify the intended beneficiaries of the NDIS by distinguishing between applicants whose needs are most appropriately and effectively met through treatments in the health and mental health systems rather than disability supports.
Under the NDIS Rules, an impairment is permanent when there are no known, evidence-based treatments likely to remedy it. But terms such as ‘remedy’, ‘available’, and ‘appropriate’ are not clearly defined, creating uncertainty in how the Rules are applied.
This uncertainty was compounded by the 2022 Federal Court decision in NDIA v Davis, which ruled that ‘remedy’ should mean a near-total cure, and ‘available’ should refer to treatments a person can realistically access and afford, not just those that exist. Because Full Federal Court decisions are binding, this interpretation could significantly widen eligibility.90Federal Court of Australia (2022).
The result is that many people with chronic health and mental health conditions – such as arthritis, diabetes, PTSD, or anorexia nervosa – could qualify for the NDIS, not because their needs are best met through disability supports, but because they lack access to affordable health and mental health care.
While these are all important needs to be met, meeting them through the NDIS blurs the line between health and disability systems and invites cost shifting from health budgets to the NDIS — a trend that risks further undermining the scheme’s long-term sustainability.
Strengthen the permanence criteria
The NDIS Act and Rules should be amended to clarify that ‘remedy’ should mean ‘substantially alleviate’ rather than ‘cure’, and that ‘available’ treatments should mean ‘generally available’.
Whether a treatment is affordable to an applicant should not be a factor in considering their NDIS eligibility, since disability supports are not a substitute for clinical treatment.
The NDIA should work with experts in the field and people with lived experience to develop guidance to help health professionals to apply consistent logic when determining the permanence of episodic psychosocial disability for the purposes of accessing the NDIS, relating to the severity, frequency, and duration of an applicant’s condition.
2.4 It is difficult to measure function
Beyond permanence, access to the NDIS depends on the extent to which an impairment results in substantially reduced functional capacity in one or more of the domains included in the NDIS Act.
The NDIS uses six domains of function: communication, mobility, social interaction, self-care, learning, and self-management.
The NDIA lists 18 preferred assessment tools for measuring functional capacity for different disabilities.91NDIA (2024g). This is necessary because no single tool can effectively measure function across all disability types.92Productivity Commission (2011, p. 315). However, in practice, assessment information is often inconsistent, incomplete, or even missing.93NDIS Review (2023a, pp. 215–17).
The current assessment tools also leave gaps in measuring function across all the required domains, which may lead to underestimating or missing people’s needs.94NDIA (2020a, pp. 12–13). As a result, many decisions are based primarily on narrative descriptions of function from treating health professionals.
The lack of a clear definition for ‘substantially reduced’ function, combined with reliance on disability-specific tools, means there is no consistent threshold for determining eligibility for the NDIS that can be applied across all applicants.
2.4.1 Diagnosis lists have contributed to higher than expected numbers of people in the NDIS
To ease operational challenges associated with high intake volumes during the transition to the NDIS, the NDIA uses access lists based on diagnosis to short-cut eligibility decision making. This means certain diagnoses are fast-tracked for entry under the disability requirements, without the need to provide further evidence.95NDIA (2022d).
Diagnosis lists are contrary to the NDIS legislation and have meant that applicants can have very different eligibility experiences and determinations even though their impairments result in equally reduced function.96NDIS Review (2023a, pp. 221–222). The lists undermine fair and equitable access decision making, which threatens the sustainability of the NDIS.
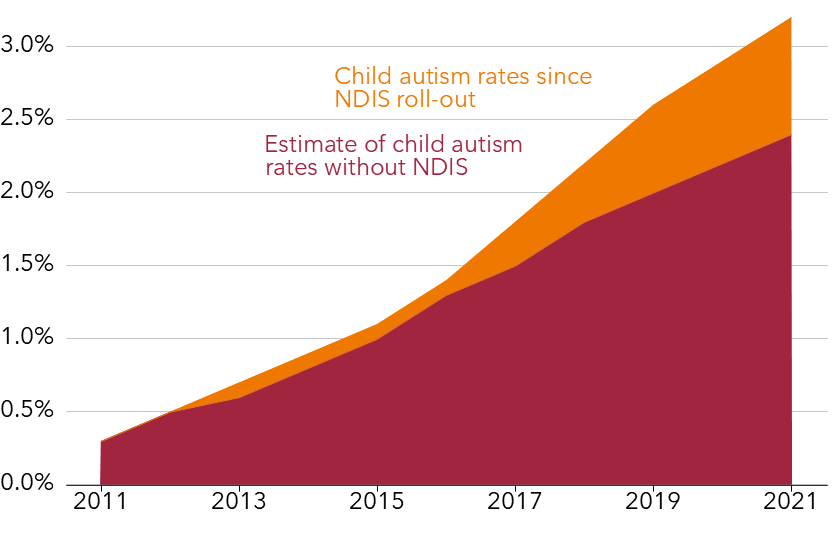
Recent research indicates that the roll-out of the NDIS from 2013 to 2021 resulted in a total reported child autism prevalence that was 32 per cent higher compared to what child autism rates would have been if the NDIS had not been introduced (Figure 2.2). Strikingly, this research points to the NDIS being responsible for almost half (47 per cent) of new diagnoses since 2013 among children aged up to 14.97Ranjan and Breunig (2025).
Autistic children were 29 per cent of people in the NDIS, and made up more than half of all children in the scheme, in March 2025.98Where children are participants aged 0-18 years. See NDIA (2025b, Table 8). And they tend to stay in the scheme. So while the average payments per autistic child are relatively low, at about $36,000 per year99NDIA (2024h, Table 1). compared to about $66,000 per year overall,100NDIA (2024c, Supplement E, Table E103). over the course of their lifetime their supports could cost $2.19 million on average.101NDIA (2023c, p. 103).
A lack of other service options may have contributed to higher-than expected numbers of diagnoses by practitioners who are motivated to ensure children and families have their ‘ticket’ to NDIS services, particularly in cases where families cannot afford or cannot access allied health services through Medicare.102Noting that some diagnoses in List A would be very difficult to falsely assign someone, such as genetic conditions resulting in severe intellectual and physical impairments, and are much less likely to be excessively diagnosed for the reasons listed here.
Figure 2.2: In the first eight years after the NDIS began, autism rates among children increased by nearly a third
Reported child autism prevalence and counterfactual estimate of child autism prevalence, 2011-2021
Note: The NDIS began a staggered roll-out in 2013, and reached ‘full scheme’ in July Ranjan and Breunig (2025) note that the counterfactual estimate of child autism prevalence without the NDIS is consistent with estimates of reported child autism prevalence in the United States and the United Kingdom. Source: Ranjan and Breunig (ibid).
Another, more concerning incentive is financial: service providers can benefit by getting clients into the NDIS and then charging the scheme for their services. Research from the Australian National University highlights anecdotal evidence of a new business model, where providers trade diagnoses for ongoing service provision.103Ranjan and Breunig (2025, pp. 26–27).
This undermines the credibility of diagnoses from health professionals. The right policy response is to ensure that diagnoses are not the main factor when determining eligibility for individualised funding.104Chapter 3 explains how government can better allocate NDIS funding based on needs assessments, and not only evidence from treating professionals.
It isn’t clear which of these, or other, incentives is more forcefully at work in pushing up the number of autistic children entering the NDIS. However, the automatic entry that List A provides for autism Level 2 or 3 is too weak an eligibility criteria to guard the NDIS against high demand for services. As a result, the NDIA cannot be confident that the scheme is covering only those it is intended to cover.
Remove the Lists and standardise functional assessments
Current NDIS access Lists should be removed, harmonising the requirement that functional capacity, not diagnosis, is the material consideration in determining eligibility for all applicants as required under the legislation. While access can and should still be fast-tracked for applicants with clear and obvious life-long disabilities, information on function should still be required to improve scheme data and for its subsequent use in planning.
Previous attempts to improve assessment of function in the NDIS have failed, notably in 2021 when the Morrison government shelved reform attempts due to fierce opposition to the proposed approach.105Department of Social Services (2021a).
Current work by the NDIA in response to recommendations of the 2023 NDIS Review to establish a standardised process of needs assessment for budget setting will not measure function and will therefore have no impact on improving access decision-making.
A separate process should be initiated to improve functional capacity assessment that can help improve consistency in access decision making.
The government should establish an appropriately skilled and equipped Taskforce with a mandate to provide advice on the design and implementation of a new eligibility assessment model.
The Taskforce should comprise experts in the field of assessment and the International Classification of Functioning (ICF), which is the international standard for defining and measuring disability, allied health professionals, government, and the disability community.
By January 2026, the Taskforce should advise on:
A clear and implementable definition of substantially reduced functional capacity, for inclusion in the NDIS Rules;
Optimal assessment design and the selection of valid and reliable tools, mapped to the ICF domains and including personal and environmental factors;
The most applicable and appropriate use of functional assessment in measuring impairment resulting from psychosocial disability, including whether this should be a material input to access decision making.
The broader utility of functional information for NDIS decision making, including for planning purposes (see Chapter 3).
Workforce and training considerations, and implementation feasibility.
Commissioning options to ensure equity of access for prospective applicants.
2.5 The NDIS is not the right service system for some applicants
A clearer distinction between the NDIS and other service systems is essential to ensure people get support from the system best equipped to meet their needs. Yet no workable test of this currently exists for NDIS applicants seeking access under the disability requirements.
Amendments to the NDIS Act, passed in 2024, introduced the new concept of ‘NDIS supports’, with a lengthy list of ‘ins and outs’ that define what is and is not an NDIS support. While this adds some specificity to the consideration of whether someone needs ‘NDIS supports’ for their lifetime, it is unlikely this will act as a firmer boundary, since the identification of a single NDIS support that might benefit an applicant would be sufficient for them to be granted access.
This change has been operational since October 2024, but is unlikely to impact on access trends. This is because there is often little material distinction in the service offering of the NDIS and the health system for some applicants. Examples would be health’s responsibility under the APTOS to provide care and support under end-of-life care programs, or to provide aids, equipment, and therapy to help someone manage a chronic health condition.106Council of Australian Governments Disability Reform Council (2015b, pp. 3–4). Considered in a different context, these types of support are frequently provided to disabled people through the NDIS.
A more meaningful distinction between the two systems is made when considering the purpose for which a service is rendered. Eligibility tests that look at a narrow set of needs-based criteria are not adequate when the goal of the service is to promote participation.
In this context, eligibility criteria should consider not only the needs to be met, but also ‘to what end?’107Klein et al note that: ‘There is an increasing realisation that service delivery based on functioning and participation considerations rather than diagnostic labels is more appropriate in a system supporting individuals with disabilities’: Klein and Kraus de Camargo (2018, p. 3). There is no textual basis to support this vital consideration in the current NDIS disability requirements.108Ernst and Young, in its 2015 independent review, recommended changes to the NDIS Act to include consideration of whether the NDIS is the most appropriate system to meet a person’s needs, to provide clarity on how the disability requirements are intended to operate for people with chronic health conditions. Governments agreed to this change, but it was never made: Department of Social Services (2017).
Strengthen criteria to distinguish the purpose of NDIS support
The NDIS Act and Rules should be amended to more effectively enable consideration of whether the NDIS is the most appropriate service system to meet an applicant’s needs. Consistent with the objects and principles of the NDIS Act, the purpose of providing disability supports is to support the person’s independence and social and economic participation.
The Rules should prescribe specific circumstances where a person’s needs are not best met through the NDIS but through the health system, with reference to the purpose for which the support is provided.
An applicant’s prognosis should be a relevant consideration for the provision of lifelong disability supports, because people with terminal conditions should not de facto become the responsibility of the NDIS rather than the health system as their health deteriorates.
2.6 The NDIS is different to aged care
The NDIS was specifically designed to target the needs of younger people whose disability was not acquired as part of the natural process of ageing.109The Disability Investment Group that advised government on the terms of reference for the original 2011 NDIS Productivity Commission inquiry specifically defined the scope of the proposed scheme as replacing ‘the existing system funding for the eligible population’, being that defined under the Commonwealth, State, and Territory Disability Agreement, which funded people with a severe or profound core-activity limitation, as defined by ABS, with age at onset up to age 65: PwC (2009, pp. 5–6). The scheme was intended to help build the capacity of people who had sustained a disability to participate as contributing members of the community and economy. The care needs of older Australians are different, typically related to managing deteriorating health.
The logic behind the age cut-off is that risk-pooling for insurance purposes focuses on rare, unexpected, and higher-impact events rather than on events of higher prevalence and which are largely predictable.110Productivity Commission (2011, p. 13). There is also an economic rationale: that people who acquire a disability later in life will frequently have the means to meet their needs, which explains the means testing of aged care versus the absence of means testing in the NDIS (see Box 2 for an explanation of why means testing wouldn’t make sense in the NDIS).111The Aged Care Taskforce concluded that superannuation trends, combined with high asset wealth, mean older people increasingly have accumulated wealth when they need aged care services, so there is more scope for older people to contribute to their aged care costs: Department of Health, Disability, and Ageing (2024b, p. 9)
The NDIS Act provides for disabled people to voluntarily move to the aged care system once they are 65, but in practice very few people make this choice because the financial incentives are stronger to stay in the NDIS.112NDIS Review (2023a, p. 181).On average, a person with disability aged over 65 will receive $132,400 per year in the NDIS, but only up to $62,075 from a Level 4 Home Care Package in the Aged Care System.113Figures are in 2024-25 dollars. See NDIA (2024a, p. 95) and Department of Health, Disability, and Ageing (2025a).
Maintain current age limits
The current age limits in the NDIS Act, which require applicants to be younger than 65 at the point of their application, should be retained.114The transition from NDIS to the aged care system is a difficult policy problem, especially for people who have been (or will have been) in the NDIS for most of their adult lives, and in particular for those who receive Supported Independent Living support. With an ageing population, this represents a significant risk to the sustainability of the NDIS in future. This policy issue needs more thinking about solutions for the long term that interact with the aged care system, although this is beyond the scope of this report.
Extending eligibility to people older than 65 would probably result in a significant influx of older Australians seeking more comprehensive supports, which would dramatically change the NDIS’s insurance dynamic towards more generic care provision. Such an expansion in liabilities should be avoided. The deficiencies in the aged care system should be remedied by reforms within that system rather than by extending the NDIS.
Box 2: Why it’s not worth introducing means-testing in the NDIS
With the NDIS costing more than expected, some have suggested means-testing could help to make the scheme sustainable.aKehoe (2022), and Ison (2023).
Means-testing is one way that governments can lower their expenditure, by shifting some costs to people using a service. It is quite common in Australian safety net programs. Social insurance programs tend not to be means-tested, for example health insurance through Medicare for Australian citizens and certain visa-holders, although income support programs such as the Age Pension and the Disability Support Pension are means-tested payments.bServices Australia (2022), Services Australia (2023), and Services Australia (2024a).
However, means-testing is unlikely to make the NDIS more affordable, for two main reasons.
First, the disabled population tends to earn less than the broader Australian population.cThe Independent Review of the NDIS ruled out means-testing and co-payments on this basis. See NDIS Review (2023a, pp. 1158–1159). About two-thirds of Australians with disability (66 per cent) are in the lowest three income quintiles, compared to less than half of Australians without disability (47 per cent).dABS (2024b). And survey data show that people in the NDIS tend to have very low incomes, with about 20 per cent of those surveyed living in poverty, more than double the rate of those surveyed who are not in the NDIS.eWilkins et al (2023).
At the other end of the income spectrum, only 7 per cent of people in the NDIS are in the top income quintile, compared to nearly 22 per cent of people not in the NDIS.fIbid (pp. 183–188). These numbers suggest that even a well-targeted means-test probably wouldn’t yield many savings.gAlthough some services through Medicare are free, Australians sometimes pay a co-payment, which reduces demand by increasing the cost for consumers. It is possible that a capped co-payment could create a degree of price incentive for people with disability, which is currently absent from the NDIS due to the scheme providing ‘first-dollar coverage’.
The government could means-test families and carers, instead of means-testing the disabled person. But this would raise questions of fairness, such as whether the parents or siblings of adults with severe disability should be means-tested for the plans their adult children or siblings receive, especially given that the federal government typically does not account for parental or sibling income when assessing a person’s eligibility for the Disability Support Pension, for example.hServices Australia (2025).
And while some wealthy families could more easily support their disabled adult relatives than most Australians, it is not clear that the benefits of targeting these families would outweigh the costs.
Second, the Productivity Commission ruled out means-testing when it proposed the NDIS in 2011, on the basis that means-testing would act as a disincentive on a population that already faces work disincentives.iProductivity Commission (2011). For example, disabled people who start to work because of the supports they receive from the NDIS could have to pay for those supports once they start working, potentially threatening their ability to afford support, while also threatening their employment. This is counter-productive when an overall aim of the scheme is to increase economic participation.
2.7 The early intervention criteria in the NDIS are not working
The early intervention criteria are intended to delineate a different approach for specific groups that could benefit from early intervention supports, including children with developmental delay or disability, and people with newly acquired disabilities or degenerative conditions.115Productivity Commission (2011, pp. 608–616).
Applicants must demonstrate that the provision of early intervention supports is likely to:
Reduce their subsequent need for disability supports in the future, and;
Improve or prevent deterioration in their functional capacity, and/or strengthen the sustainability of their informal supports (e.g. through building the capacity of family members or friends).
The NDIS Act provides no specific thresholds to assist with the consistent determination of when these criteria should apply or cease. The absence of any objective threshold for the assessment of developmental delay has meant there is a very low bar to entry under this criteria, which hinges entirely on a clinician’s judgment.
To make matters worse, there is a potential perverse incentive when the clinician who is assessing a person’s eligibility for the NDIS also stands to gain from that person getting into the scheme and spending their plan funding on the clinician’s services.
The implementation of early intervention in the NDIS has been largely age specific, not nearly early enough, and entirely detached from the other service systems it was supposed to complement, including early childhood development services, families services, and low-intensity clinical services delivered within the mental health system.
The NDIS does not have a specific approach to planning processes for adults who enter the scheme through the early intervention requirements.
The NDIS does have a specific approach to early childhood planning for children up to the age of 9, but the program design, which relies heavily on individualised funding as a pathway to medicalised supports, is not well suited to delivering what children and families actually need from early intervention.116Gavidia-Payne (2020, p. 7).
There is broad consensus about what constitutes best practice in early childhood intervention and care, with the principles of evidence-based support integrated into the mainstream settings where children live, learn, and play.117Department of Social Services (2024a, p. 10), Dimmock et al (2024), and Trembath et al (2022a). Yet the largest single source of support and funding for young children with developmental delay or disability comes through an individualised funding system that is uniquely ill-equipped to conform to these principles.118Researchers note that the service drivers of the NDIS work contrary to its own principles of supporting increased participation (Foley et al (2021, p. 3028)), as well as conflicting with effective community-based approaches to supporting disabled children (Breen et al (2011)).
An NDIS that loosely allocates money to families, who must then differentiate between therapies in the marketplace under pressure from providers rather than being directed to the early intervention support most likely to yield good results, is not the optimal way to spend public resources.119Gavidia-Payne (2020). Yet for about 167,000 Australian families,120NDIA (2025a, p. 26). this is the only option available, because the NDIS has crowded out most of the services that could work far better for their children.121Foley et al (2021, p. 3028).
Rather than a focus on developmental results for children, the focus of participants and families shifts to the amount of money they receive in a plan, and maintaining those funding levels. The market-based NDIS model has incentivised providers’ pursuit of ongoing business, often at the expense of high-quality early intervention.122Ranjan and Lowe (2023, p. 7), and Foley et al (2021, p. 3025).
Attempts to enhance the operation of the NDIS early childhood approach have failed to deliver meaningful improvements.123The NDIS introduced an early childhood early intervention approach in 2016, and initiated a ‘reset’ in 2020, informed by extensive national consultation: NDIA (2020b). Despite these efforts, the 2023 Review of the NDIS concluded that ‘the approach to supporting children with disability or developmental concerns and their families is not working’: NDIS Review (2023a, p. 388).
Legislative changes in 2024 were intended to pave the way for improvements in the early intervention pathway, but aside from people joining the NDIS now getting confirmation about what entry criteria they met, nothing has yet changed.124Parliament of Australia (2024, p. 5).
The problems with NDIS early intervention are too fundamental to be fixed through iterative policy and process improvement. For some people, including many of those who enter the NDIS through its early intervention requirements, the program design of individualised funding is never likely to deliver optimal results.
2.7.1 Foundational supports can deliver better early intervention results
Foundational supports are the right idea to save the NDIS, but the scope of their coverage for some groups is likely to be difficult to distinguish from the current early intervention requirements.
The purpose of both programs is identical, but the current early intervention and developmental delay requirements present such a low bar that people are likely to continue applying for a more expensive individualised plan than take up foundational supports. The incentive to apply to the NDIS would remain.
If the bar for eligibility into the NDIS early intervention pathway were set higher, this could help to triage applicants to the right early intervention supports – either in the NDIS or through foundational supports. However, there is no clear logic for creating two early intervention pathways, one with individualised funding – a looser, and less effective, method of allocating resources for early intervention – and one through foundational supports which uses commissioned services.
Foundational supports should be available to people who need some support but are not best served by lifelong disability support delivered through an individualised plan. This should include a range of early intervention supports of differing types and intensities.
These services should substitute for rather than duplicate the supports currently provided under the NDIS early intervention criteria – including for all people under the age of 18 with developmental delay or disability who are supported through the NDIS early intervention approach.125Note that this does not include children in the disability requirements pathway under Section 24 of the Act; namely, children with lifelong and severe disability. Grattan anticipates that adults currently in the early intervention pathway will transition to the disability requirements pathway of the NDIS under Section 24 of the Act.
Remove NDIS early intervention requirements
It has proved impossible for the NDIA to implement two very different pathways through individualised funding within the same national program in a way that delivers optimal early intervention results for people needing these supports. There is no reason to assume that the situation will improve under essentially the same policy settings as the scheme continues to grow.
NDIS eligibility criteria should be adjusted so that children with developmental delay or disability and people with psychosocial disability who need early intervention can be directed to targeted foundational supports, rather than to early intervention through an individualised funding approach.126Grattan’s analysis focuses on targeted foundational supports for children and people with psychosocial disability, but it is possible that targeted foundational supports could serve a broader group of people with disability in future; however, this is out of scope for this report.
The current early intervention criteria should be removed, to help ensure that people get access to evidence-based early intervention supports delivered in the most effective and efficient way. It would also create a more targeted individualised funding system in the NDIS, focused on people with a lifelong need for disability support. And this will be far easier for the NDIA to administer.
Chapter 3 explains how individualised plans can still be tailored to ensure that some groups needing a specific approach (perhaps within their first few years on the NDIS) can get support in the right way.
Chapter 4 explains how the new foundational supports ecosystem should work, how it should be funded, and how transition arrangements should operate.
IN THIS CHAPTER
Share
3 Fairer plans in the NDIS
Saving the NDIS requires reforming two core functions of the scheme: how budgets are set, and how disabled people plan their supports. Budget setting determines how much funding each person receives. Planning involves helping people to decide how to use that funding to get the supports they need.
Currently, the NDIS sets budgets inconsistently, offers rigid plans, and provides limited support to people during the planning process. This leads to a poor experience for many disabled people and undermines the scheme’s ability to manage claims – a key responsibility of any insurance system.
Chapter 2 outlined who should be eligible for individualised funding. This chapter sets out how the NDIS must change the way it sets budgets and supports planning, so that funding decisions are fair, consistent, flexible, and better tailored to people’s needs.
3.1 Poor claims management is threatening NDIS sustainability
The NDIS has not developed the levers it needs to effectively manage claims, and people with disability are being left to navigate a complex and inflexible bureaucracy and disability services system.
The NDIS currently sets budgets through a highly subjective and often adversarial process. It involves an NDIA planner determining which of the support items a person has requested are ‘reasonable and necessary’ for them. This involves applying a number of discrete tests in each case, including whether the requested support is likely to be beneficial, safe, and value for money.
Although people with disability and their families collect copious evidence from allied health professionals and specialists to support this process, public servants rarely have time to go through the evidence.127Parliament of Australia (2025, p. 7). This means that how much funding each person gets in their plan relies less on any evidence provided, and more on the judgment of individual planners. And this invites variability, inequity, and inconsistency into NDIS budget setting.
These thousands of decisions made by junior bureaucrats about how much funding each person receives make it difficult for the NDIA to keep plans within the annual NDIS budget.
There is also very little planning with disabled people in the NDIS. Even though the scheme is built on the promise of meeting the needs and goals of individuals with disability, so long as these are reasonable and necessary, there are in fact few opportunities for individuals to get help in planning how to use their funding, which can sometimes be in the hundreds of thousands of dollars for more complex plans.
And when people with disability get their plan, they don’t always have the flexibility they need to individualise how they spend their funding, or change how they spend their funding over the life of the plan, which can be as long as five years.
The upshot of poor claims management is that inflation in funding – both during the period of a plan (intraplan inflation) and between plans (interplan inflation) – drives scheme growth (see Figure 3.1).
Legislation passed in 2024 will help government improve its claims management, which will assist in moderating growth towards the National Cabinet’s 8 per cent annual growth target. The NDIA has already banked on $19.2 billion of savings through a range of measures introduced in 2024, including to strengthen planning processes (see Figure 3.2).
However, there is a significant risk that the government could hit the target but miss the point; in other words, reaching the savings target but in ways that are detrimental to people with disability.
That the NDIS is demand-driven is a good thing – it means that people with disability can get the reasonable and necessary supports they need. But the NDIS has to contain costs and growth, just like every other government program. Any time government decides to spend money on one program, it means that it can’t spend that dollar on another program. The opportunity cost of spending more on the NDIS gets higher as the scheme grows each year. Higher costs also strain the social licence on which the NDIS is built.128Duffy and Brown (2023, pp. 20–21), and Young (2025).
Claims management and budget-setting are two of the main levers government has to contain costs and growth in the NDIS. Instead of rationing the NDIS through increased administrative hurdles, or inadequate funding, well-implemented claims management and budget-setting can ensure that people with disability get what they need, in a way that is affordable to governments.
3.2 A sustainable NDIS needs a better planning process
Individualised funding by itself does not guarantee choice, control, and good results for people with disability.129Dickinson (2017).That requires a person-centered process that helps people plan how they will use their funding to meet their needs and pursue their goals. And yet, a genuine planning process that enables people with disability to map out how to get the most out of their funding is largely missing from the NDIS today.
Figure 3.1: Interplan and intraplan inflation are big sources of NDIS growth
Annualised percentage change in plan budgets for people in the NDIS
Source: NDIA (2024c).
Here are five steps to establish a new planning process which would ensure that, as the NDIA makes changes to moderate growth, people with disability also get better results: use standardised assessments for budget setting, allocate budgets that fit within the total funding envelope, prioritise a better planning experience, enable more flexible use of funding, and collect data to monitor and improve the process.
3.2.1 Use standardised assessments for budget setting
The current planning process is administratively complex. It itemises a list of permissible expenditure. It works this way because planning has been the primary cost control mechanism in the NDIS – a task for which it has proved woefully ill-equipped.
This is not how individualised funding systems are supposed to work. The current process of listing every single need a person has and how it will be met to create a budget from the ground up is subjective, time consuming, and leads to inconsistent funding decisions.130NDIS Review (2023a, pp. 557–561). And it doesn’t lend itself to the principles of choice and flexibility.
Worse still, some of the evidence used to support funding claims may not be reliable due to potentially perverse incentives that exist in the current system, which we described in Section 2.4.1.131Ranjan and Breunig (2025).
To save time and increase fairness, Australia should adopt a system similar to the UK’s, where resource allocation is separated from planning, so that funding entitlements are transparently connected to a standardised process of assessment that provides a budget before planning commences.132Hole et al (2024, p. 28).
Closer to home, this is not dissimilar to the new assessment and budget setting process for the Support at Home program in aged care, which transparently links a funding entitlement to a standardised assessment using validated instruments.133Department of Health, Disability, and Ageing (2025b).
Figure 3.2: The NDIA is banking on big savings from the new planning framework
Cumulative expected savings by reform, 2024-25 to 2027-28
Notes: ‘Intraplan inflation’ savings are savings expected to result from operational activities targeting intraplan inflation, including ‘via establishment of total funding amounts, funding components, and funding periods’ (NDIA (2024a, p. 6)). ‘Budget models’ savings are the savings expected to result from the implementation of new framework planning. Source: Parliament of Australia (2025).
In the NDIS, a person’s funding entitlement should reflect the expected costs of providing a reasonable and necessary package of supports for someone with a similar level of function, support needs, and environmental and personal context (see Figure 3.3).
A standardised process of assessment should be the starting point for determining a reasonable and necessary budget, or ‘benchmark budget’ (see Section 3.2.2).
The standardised assessment should be an objective process that consistently identifies and measures need in all of the domains included in the NDIS Act, and must be valid for a wide range of age groups and disabilities.
For example, standardised assessments for people with psychosocial disability will require specific attention to the complexity of assessing the support needs of this group. The functional capacity of people with psychosocial disability is often episodic, variable, and influenced by effective medication management.
Consistent with the current legislation, this process, including any tools chosen, should be mapped to the International Classification of Functioning.134See ICF Interest Group Australia (2025) for a fuller articulation of the International Classification of Functioning and its potential uses in NDIS assessment processes. Objectivity matters for ensuring that the needs assessment provides an accurate, valid, and credible measure of need.
Figure 3.3: How standardised assessment would work
Source: Grattan Institute analysis.
Recent changes to the NDIS Act provide the legislative scaffolding around which new plans will be designed in future, including the ability for funding levels to be set using objective variables derived from standardised assessment.135Parliament of Australia (2024).
This changes the significance of ‘reasonable and necessary’ as an animating concept of the NDIS. In future, ‘reasonable and necessary’ will refer to the level of funding a person gets in their plan, rather than the reasonableness or necessity of any individual support that has been agreed or declined.
These developments have the potential to significantly improve the consistency, fairness, and predictability of NDIS decision making, if well designed and implemented. This will improve results for disabled people and support the sustainability of the program.
The government should quickly develop rules to support adoption of the new planning approach, informed by technical design of the new assessment and budget-setting process by the NDIA.
Government should also make two important changes to the currently proposed settings: incorporating functional assessment alongside an assessment of need, and creating a more realistic implementation timeline for the new planning framework.
First, the NDIA should incorporate a functional assessment into the needs assessment process. This will mean that the same process can be used to determine people’s eligibility for the scheme as well as their plan budget. The information assessors needed for both purposes is very similar, so asking people to undergo two assessments is unnecessarily burdensome and duplicative.
Planning decisions should be directed towards addressing barriers to people’s social and economic participation that result from functional limitations, so an accurate measure of function is needed. A more comprehensive assessment could help people understand their needs, strengths, and capabilities, and the kinds of support they might need, regardless of their eligibility for individualised funding.
Second, government should confirm that the implementation timeline to commence the new framework planning transition will be pushed back to July 2026 to allow sufficient time to design the assessment process, and engage and train the workforce. September 2025 was not realistic and risks a suboptimal roll-out that would undermine public confidence in this critical change.
In this new timeline, government should also account for the integration of functional assessment within the same process, including how this aspect will be commissioned following advice received from the Taskforce established for this purpose that we propose in Chapter 2.
3.2.2 Allocate budgets that fit within the total funding envelope
Once a person with disability has had their standardised assessment, the NDIA should provide them with a benchmark budget – an amount of funding matched to the level of support needed to overcome barriers to their participation, that they can use to start planning their individual supports.
Benchmark budgets should correspond to people’s functional capacity and support needs, as well as accounting for variables such as age, remoteness, and informal support. The agency should estimate the likely spread of support needs across the NDIS population, and allocate the overall NDIS budget into benchmark ‘buckets’ for groups of individuals with disability.
The NDIA should finalise the person’s provisional budget through the planning process by identifying any specific supports that should be added. A finalised budget might include additions for capital costs, such as disability-specific goods (including assistive and custom technology, and mobility aids), home or vehicle modifications, and Specialist Disability Accommodation for which separate assessments might be required.
While there may be some variation in benchmark budget amounts that arise through appeals, the benchmark budget should generally be sufficient other than in clearly defined circumstances. The NDIA should monitor the roll-out of benchmark budgets to ensure they are sufficient and to mitigate the risk of bracket creep, and make adjustments to the benchmarks over time as needed.
Introducing benchmark budgets before the planning process will enable the NDIA to more easily allocate individual plans that stack up to the overall NDIS budget. Managing claims and the insurance pool means that individual plans should fit within the annual budget, with some room for risk, error, and flexibility for external changes such as new enterprise bargaining agreements, inflation shocks, or other changes to the price guide.
This change will allow government to calibrate more predictable funding decisions, and more easily keep the scheme’s overall costs within annual budget parameters. For the first time in the NDIS, there would be a golden thread between individual funding allocations and the overall funding envelope.
Benchmark budgets that are based on need should also help the NDIA to prevent excessive interplan inflation, which is common with the current planning approach (see Figure 3.1).
Introducing standardised assessments that link to benchmark budgets should create a fairer and more predictable NDIS – responsive to demand, but with far better tools to manage claims. A robust needs assessment that ties to benchmark budgets, and a more personalised planning process, would also enhance disabled peoples experience of, and confidence in, the NDIS.
3.2.3 Prioritise a better planning experience
By making resource allocation a separate step to planning, there is an opportunity to plug a yawning gap in scheme design.
In future, rather than being a negotiation around what services will be funded, the planning process should be focused on helping the person explore how to best use their formal and informal resources to meet their needs and pursue their goals.
Setting the budget in this way will shift peoples’ focus to planning within a budget, with the emphasis on getting the best results rather than securing a higher dollar amount.
Systems of self-directed disability support the world over have tended towards resource allocation methods which ensure the eligible person has an early indication of the funding available to meet their needs, before the planning process starts.136Alakeson (2010, p. 2).
Giving people a benchmark budget before they plan their supports makes sense for three main reasons:
A transparent funding entitlement system that gives people a budget from the start shifts the power dynamic away from professionals and toward people with disability, because funding is no longer primarily down to the professionals’ judgment.137Duffy (2007, p. 8).
It is easier for people with disability and their family to plan when they know what funding is available to them at the start of the process.138See, for example 11.23 in UK Department of Health and Social Care (2025, pp. 155–156).
People with disability will have greater autonomy and self-determination over their supports if their budget is not tied to hours of support or line-items, as happens today.139Duffy (2005).
The planning process should be holistic, considering all of the resources available to the person, rather than only looking at how funding is used. The plan should have regard to how mainstream services and community-based and/or unpaid support can contribute to meeting needs in addition to any specialised supports.
Within this model people should be free to plan in a way that best meets their needs, with support from a wide range of sources. For example, from family or friends, from peers, from a disability organisation that understands their needs, or in future with the support of a navigator as envisaged by the 2023 NDIS Review.140NDIS Review (2023a, pp. 313–343).
The planning process should happen as close as possible to the person and their community. Navigators who understand local circumstances and have strong relationships with community organisations and providers will be best placed to help people get the right support.
In our 2024 report on how to reform NDIS housing and support, we proposed a range of functions for specialist navigators. This included helping disabled people to set goals, build their knowledge and expectations, widen and sustain their informal networks, and connect with community organisations, providers, and other government services.141Bennett and Orban (2024a, pp. 39–40).
But not everyone will need a navigator or help to plan. When planning is no longer a process of government resource allocation, it does not need to be a task dominated by NDIA bureaucrats. As the NDIA employs more assessors and is able to provide funding entitlements based on this process, fewer ‘government planners’ will be needed.
It is conceivable that, with a range of other well-supported choices available, most peoples’ plans will need no further input from the NDIA. This will reduce administrative costs and enable the government to shift staffing resources to the more complex end of need, where a more hands-on role in case management, safeguarding, and specialised planning is needed.
3.2.4 Enable more flexible use of funding
Under this new planning approach, individualisation comes from how and where people choose to spend their funding, rather than the individual items agreed to in the plan.
The NDIS should allow many people with disability greater flexibility in how they choose to use their plans. The evidence is clear that the most successful individualised funding schemes enable people to be creative and flexible, and make their own decisions day-to-day about how they are supported.142Fleming et al (2019), Laragy (2010), and NDIA (2022e).
More flexibility enables people with disability, as experts in their conditions, to spend their funding entitlements on goods and services that suit their individual needs, goals, and circumstances.
The NDIS does need spending guardrails, but it is the new planning framework that will do the heavy lifting on controlling costs in the reformed system, rather than a list of permissible support items. Grattan Institute has previously argued that when the NDIA is confident that it is setting budgets correctly at the ‘front door’ in a way that fits within the funding set by government, barricading the ‘back door’ with extensive rules on spending is unnecessary and counterproductive.143Bennett (2024, p. 3).
The NDIS does not need a Medicare Benefits Schedule for disability that extensively codifies everything that can bought with NDIS funding. The objectives of increasing people’s social and economic participation are not the same as the objectives of medical treatment, and don’t lend themselves to similar policy settings.
Rather than reducing growth in the cost of the NDIS, the lists are more likely to temporarily reduce how much of their plans people spend (that is, a drop in plan utilisation rates); however, this effect would disappear once people start to substitute prohibited supports with permitted supports.
Our proposals in Chapter 2 to remove the early intervention pathway clarify the focus of the remaining individualised funding system, to which the lists would apply, as being a system of self-directed support for people with lifelong disability, within the framework of the UN Convention on the Rights of Persons with Disabilities.
Formal constraints on flexibility should be a sparingly used feature of any such system. Self-directed support systems operate best with the minimum hard exclusions and a permissive, principles-based framework that optimises flexibility day-to-day. This is reflected in statutory guidance in the UK which explicitly discourages the use of lists of allowable purchases, since the range of possibilities should be very wide and beyond what can be listed at any point in time.144UK Department of Health and Social Care (2025, Section 10.48).
Disabled people needing lifetime support will often be well placed to make the most effective and efficient decisions about the supports they buy. But more should be done to support this process so that people have easy access to relevant evidence and supports to assist with their decision making where these are required.145The NDIA should fully implement its Supported Decision Making policy to expand access to these supports: NDIA (2023d).
The federal government should rethink the current ‘in and out’ lists contained in the interim Section 10 Rules that now govern the use of NDIS funds. The current rules are unnecessarily complex, overbearing, bureaucratically burdensome, and will prove impossible for the NDIA to properly police.146Previous abandoned attempts to reform the NDIS approach to planning and budget setting in 2021 did not include a proposed expansion of rules restricting the use of NDIS funds. To the contrary, consultation materials relating to proposed reforms stated: “Once we have improved the way we build budgets, plans can be much more flexible, without an increase in rules…that could impact on participant choice and control. We will have fewer rules but more consistent overall total budgets to support participants to pursue their goals:” NDIA (2021a, p. 15).
The current rules could also have a chilling effect on much-needed innovation, for example by undermining the viability of cost-effective alternatives to expensive housing and living supports.147As recommended by Grattan Institute in Bennett and Orban (2024a).
The government should work with the disability community on a replacement Rule. The new Rule should reflect the overall policy objectives of these changes: to ensure sustainable resource allocation while enhancing people’s planning experience and flexibility. The new Rule should ensure that NDIS spending is in line with community expectations. It should be introduced in parallel with the commencement of the new planning framework transition from July 2026.
3.2.5 Collect data to monitor and improve the process
Changing how budgets are allocated, reforming the planning process, and altering how people can use their plans are substantial changes to the NDIS. The NDIA should collect more data so it can evaluate these reforms, track the budget impact and has the information it needs to run the NDIS as an efficient insurance scheme. Such data are also essential for independent prudential governance, a principle of insurance systems.148Walsh and Johnson (2013, pp. 330–331).
With any needs assessments and budget allocation process, there is a risk of misallocation. If people with disability receive less funding than they should (a lower benchmark budget than is appropriate for their needs), then they will miss out on services and supports that they need to live safely, to participate in the economy and community, and which could help to reduce the impact of their disability in the long run.
On the other hand, if people with disability receive more funding than they should (a higher benchmark budget than is appropriate), they may receive services and supports that are of little benefit to them, when this money could have been used to support other people with disability.
To ensure the new budget setting and planning system is fair, accurate, and consistent, the NDIA will need to collect consistent and in-depth data on:
needs assessment results by assessor;
benchmark budget allocations resulting from these assessments;
any socio-economic inequities in assessment results or budget allocation;
the frequency of, reasons for, and results from people with disability requesting alterations or additions to their budgets;
the impact of appeals on budget increases over time; and
how the cost of all claims, including any adjustments to benchmark budgets, stack up against actuarial projections in the context of the total NDIS budget (or the ‘aggregate premium’).
These data will help the agency to better run the NDIS, including adjusting budget benchmarks and informing training for assessors. As such, it will be important that benchmarks can be adjusted in response to scheme experience, particularly as the new system beds down and evolves, rather than being locked down in legislation that is far more difficult to change.
Robust, detailed, and informative data regarding the results of the NDIS for its beneficiaries has been long missing from the NDIS. The current outcomes survey is high-level and provides little information to assess the effectiveness of supports and services in the NDIS.
An insurance scheme needs better outcomes measurement to understand which supports are the most effective for which populations. The NDIA and researchers should use this data to improve the scheme for people with disability and their families, and to make the NDIS more efficient and equitable.149For example, by assessing the socially optimal quantity of disability insurance.
Work undertaken since 2021 by the NDIA with external researchers to develop and validate a preference-based well-being index to routinely measure and monitor disabled peoples’ experience with the NDIS should now be implemented.150Monash University Centre for health economics (2023).
The current NDIS outcomes framework should also be reviewed, to identify areas for improvement aligned with the introduction of new assessment, budget setting, and planning processes. Data should include longitudinal surveys of the NDIS population, as well as sample panel data and other surveys of samples of interest that would benefit the NDIA and people with disability.
The National Disability Data Asset also promises to link data across federal, state, and territory governments to other administrative datasets, to give a clearer picture of the lives of people with disability.151Australian Government (2025). More data collection by the NDIA will strengthen this data asset, allowing the agency to better run the NDIS, and independent researchers to better scrutinise its results.152Data collection should also cover foundational supports. See section 5.4.2 for a discussion of data collection across the disability services system under Grattan’s plan.
3.3 The role of stated supports and funding limits
While flexibility should be the general rule, in some circumstances there will be good reasons to provide more prescriptive funding.
A ‘stated support’ is where a support is described specifically in a person’s plan, with the effect that funding allocated to it can only be spent in the way described, and not used flexibly or on other things.
Since our proposals in Section 2.7.1 involve removal of the early intervention criteria, the ability to state supports will be an important remaining lever to manage risk and require the use of specific supports where that is warranted and appropriate.
Stated supports should include funding allocated for capital items, such as assistive technologies or home modifications, because these are often high cost and not generally substitutable. Other supports such as positive behaviour supports and Specialist Disability Accommodation (SDA) should also be quarantined. This is because of the high risk of substituting highly customised accommodation for people with extreme functional impairments, with other less-appropriate supports, and the fact that the SDA system is still maturing and investors need predictability around returns.153Bennett and Orban (2024a, pp. 38–39).
The use of stated supports should also be calibrated to ensure particular groups of eligible disabled people get access to specific evidence-based supports or therapies where there are compelling reasons for such tailoring. Examples would include:
people entering the NDIS with a psychosocial disability – where stating specific recovery oriented services and intensive case management or support coordination could promote recovery;
children and young people with disability who could benefit from specific individual or family capacity building;
people planning for an important life-stage transition, where quarantined funding to explore housing and support options or to start thinking about leaving school and entering the workforce could ensure they can get specialised advice and support;
people with newly-acquired disabilities, such as spinal cord injury or acquired brain injury, who could benefit from specific therapies, supports or goods.
Measuring the impact of the use of stated supports could enable some flexibility in the intensity of support provided over time. This could include the use of zero-dollar plans for people with fluctuating or episodic needs whose support might be dialed up and down as needed without affecting their ongoing eligibility status.
The NDIA should develop rules that determine when plans can include more prescriptive stated supports and zero-dollar plans. Such rules should not unduly restrict peoples’ support arrangements or undermine creativity and innovation.154Ibid.
Consideration should also be given to the sparing use of support category limits that would operate as ceilings on the use of particular supports and services in some circumstances. For example, in relation to certain therapies where there are concerns that the excessive intensity of an intervention could reduce a child’s ability to be included in ordinary school and community life.
3.4 The importance of innovation for high-cost plans
One of the NDIS’s most important responsibilities is to provide support to Australians with disability who need extensive help at home with everyday activities.
Supports in this part of the scheme are costly. Grattan Institute research showed that about 40 per cent of NDIS costs cover supports for about 7 per cent of people in the NDIS.155Ibid.
The average payment to someone who has a profound disability and needs Supported Independent Living (SIL) funding for supports at home is $430,500 per year, as of 31 March, 2025.156NDIA (2025a, p. 67). Since 2023, total payments to people with SIL funding has increased by 19 per cent per year on average, and the number of people getting SIL funding has increased by 8 per cent per year on average.157Ibid (p. 67).
This part of the NDIS is crying out for innovation, but there have been few changes in the way these services operate since the inception of the NDIS.158NDIS Review (2023a, p. 591). Most people with this level of need are still living in group homes, where the high costs also come with high risks of violence, abuse, neglect, and exploitation.159Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (2023, ch. 9, vol. 7), and NDIS Quality and Safeguards Commission (2023, pp. 42–62).
Our proposals in Chapter 2 to remove early intervention criteria and create a more targeted individualised funding system for people with a lifelong disability will enable a long overdue, more concerted focus on driving innovation and improving results for people with the highest needs.
There are better and cheaper alternatives to group homes, but they are not widely available, in part because NDIS policies are too rigid and its funding too inflexible. Other countries, including the UK, the US, and Canada, have introduced reforms to disability housing, including new living arrangements which offer people greater choice and a more individualised approach.160Bennett and Orban (2024a).
Grattan Institute research showed that some alternatives – which we called Individualised Living Arrangements (ILAs) – can cost the same or less than group homes.161Ibid (pp. 22–23).
This is backed up by other recent research that also indicates that ILA’s can cost between 9 per cent and 45 per cent less per person, per year than a comparable group home arrangement. This research indicates that government could achieve a saving of about $260 million over five years if 500 more people each year chose to be supported in these arrangements rather than in group homes.162Burke et al (2025, p. 5).
The NDIA should prioritise giving more support to these arrangements that are already working well in Western Australia and overseas, and will help more disabled people into ordinary housing in the community for the same or less money than current services.
Identifying the best ways to offer intensive supports is in keeping with the NDIS’s insurance principles and justifies investment in research and trials to test, evaluate, and implement other promising approaches.
Innovation is needed in housing, in the way support is provided, and in the way technology is used in these settings.163For example, research conducted in Japanese nursing homes showed that robotic technology can automate certain tasks, freeing up support workers for tasks that needs empathy, human touch, and dexterity. The evidence indicates that the nursing homes that use robots to monitor residents offer higher-quality care, greater productivity, and lower attrition among care workers, which reduces staff turnover costs: Lee et al (2025). Grattan Institute’s previous research identified promising examples in each of these areas that individually or in combination could offer cost-effective alternatives for disabled Australians who need the most support.164Bennett and Orban (2024a, pp. 16–17), and Morgan et al (2024).
The NDIA should also consider how it can offer housing and living supports effectively and efficiently to people with disability at the margin of eligibility for Supported Independent Living (SIL) funding.165Grattan Institute analysis of unpublished NDIA data shows there are tens of thousands of disabled people who need extensive support at home who are funded for six or more hours per day of Assistance with Daily Life: Bennett and Orban (2024a). The high costs of intensive housing and living support means that the Agency needs to carefully manage eligibility for these supports. However, there has been little innovation so far in service offerings to people with disability at the foot of this ‘funding cliff.’
Beyond the scope of current initiatives earmarked for savings to moderate growth in the NDIS to 8 per cent, a more concerted focus on driving innovation in the scheme, particularly for high-cost plans, should form part of the government’s thinking. Innovation in this part of the NDIS could improve the lives of disabled Australians who need the most support from the scheme, and it could help make the scheme sustainable. Grattan Institute has previously recommended that the federal government establish an NDIS innovation fund to trial and spread individualised living arrangements and optimise the use of technology in delivering cost effective in-home supports.166This proposal was costed in our report Better, safer, more sustainable: How to reform NDIS housing and supports, with costs anticipated to be offset by savings resulting from cheaper support options being chosen over time. As such this proposal is not costed again in the context of our proposals in this report: Bennett and Orban (ibid).
IN THIS CHAPTER
Share
4 Rebalancing the NDIS and disability services
A sustainable NDIS requires more than individualised funding – it needs a strong foundation of general and targeted supports for people with disability. Crucially, this can be achieved without new funding.
Today, many people with disability who do not qualify for individualised NDIS funding have very limited access to alternative supports. This creates strong incentives to seek entry to the scheme, even when it may not be the best fit for their needs.
The gap is particularly clear for children with developmental delay or disability, where individualised funding is often the only available pathway, despite its limited success in delivering early intervention. People with psychosocial disability – the fourth largest group in the NDIS – also face challenges in a system overly reliant on individualised plans.
Foundational supports can help rebalance the system. By offering the right services at the right time and in the right way, governments can better meet people’s needs and reduce pressure on the NDIS to provide everything for everyone through an individualised plan.
This is not a question of spending more. Our analysis shows the problem lies in how existing funding is allocated. Governments can meet their commitment to foundational supports by redirecting a portion of their existing NDIS contributions.
Governments should jointly commission general and targeted foundational supports that offer a viable alternative to individualised plans. Over a five-year transition, some cohorts should transition to having their support needs met exclusively by targeted foundational supports, and all NDIS participants should transition to receiving some service types through general foundational supports.
4.1 Foundational supports are the ‘missing middle’ of NDIS services
Foundational supports are part of the NDIS design, yet they have never been fully or properly funded or implemented. At the scheme’s inception, the Productivity Commission envisioned that the NDIS would have three levels of ‘coverage’:167Productivity Commission (2011).
All Australians under 65 are covered by disability insurance (i.e. the NDIS) that is there if they need it.
All Australians with disability (about 21 per cent of the population)168ABS (2024b).have access to some low-to-mid-level disability-specific supports and services if they need them.
Australians with permanent and severe disability who need intensive supports receive individualised funding to meet their needs and pursue their goals.
Foundational supports is the new name the 2023 NDIS Review gave to the second level of coverage in Australian disability services.
Even though the NDIS has become synonymous with individualised funding, the third level of coverage, that was never supposed to be the only game in town.
Foundational supports can be an efficient way to deliver services to many Australians with disability who need some support but do not qualify for individualised funding.
But these supports are mostly absent in Australia today.
When this second tier of coverage was originally conceived, it was considered a key function of the NDIS in providing information, linkages, and capacity building services — the ILC Program.169Council of Australian Governments Disability Reform Council (2015a).
But investment in these supports has consistently declined as a proportion of total funding, from an already low base (see Figure 4.1).170Note that a very small funding uplift was announced in the 2025 Budget, but this will not be sufficient to reverse the trend. For example, in 2028-29, ILC funding is budgeted to be $150 million per year, just 0.2 per cent of the projected expenditure on NDIS individualised payments: Commonwealth of Australia (2025b) and NDIA (2024a).
And since the start of the scheme, the disability-specific supports that were meant to be linked and referred to have largely fallen away. This means that the existing foundational supports system has all the utility of Uber Eats with no restaurants enrolled.
The task to build up foundational supports, therefore, is bigger and more complex than it was in 2011. It consists of building an effective system of information, linkages, and referrals (general foundational supports) and re-establishing non-NDIS disability-specific supports for particular groups of disabled people (targeted foundational supports).
While the original idea has evolved over time, it is still the right one. The existence and efficacy of foundational supports remains one of the only plausible ways that the gravitational pull of unmet need towards an increasingly unsustainable NDIS can be avoided.
4.1.1 The lack of foundational supports puts pressure on the NDIS to deliver everything for everyone
In the absence of foundational supports, people with disability have, understandably, been eager to get individualised funding.
Figure 4.1: Spending on Information, Linkages, and Capacity Building is declining as a proportion of total funding
Expenditure on ILC as a percentage of what was spent on NDIS individualised payments each year
Notes: ILC funding is not included in the total payments; percentage is to illustrate the relative scale only. ILC expenditure includes ILC grants and the 20 per cent of Partners in the Community funding that is allocated to ILC-related activities. For further information about how this ratio was calculated, see Appendix B. Sources: See Appendix B.
Individualised funding is the most intensive form of disability insurance in the NDIS, designed to support people with lifelong and severe disability. It intends to provide people who need specialised disability support the opportunity to control their services and make choices about the support they need, with or without assistance from family, friends, and advocates.171Individualised funding, by many different names, emerged as a result of extensive advocacy from the disability community in the US, UK, and Australia who wanted to have more control over their supports, including the option to move away from institutional support models.
For example, an adult with moderate or severe intellectual disability who needs around-the-clock assistance at home or to go out into the community; or a person with an acquired physical disability who lives with their spouse and children, and needs a support worker to get in and out of bed, shower, and use the bathroom to get ready for work. People with severe and profound disability make up about 10 per cent of the disabled population in Australia.172Based on the Productivity Commission’s estimate of those eligible for the NDIS (410,000 people eligible for the NDIS based on a disabled population of 4 million people in 2009). See Productivity Commission (2011, pp. 14–15).
But without appropriate alternative supports, there have been increasing numbers of applicants and entrants to the NDIS, including some people for whom timely access to evidence-based programs of support, accurate information, advocacy services, and some types of assistive technology could meet their support or early intervention needs, without the need for individualised funding.
These people could have their needs met in a simpler, more cost effective way through general and/or targeted foundational supports if they were available.
Experience has shown that an NDIS program design that has become solely reliant on individualised funding is particularly poorly suited to the needs of children with developmental delay or disability who require early childhood intervention and support, and people with psychosocial disability.173Note that although this chapter focuses on targeted foundational supports for children and people with psychosocial disability, it is possible that targeted foundational supports could serve a broader group of people with disability in future; however, this is out of scope for this report. Grattan Institute proposes that these two groups should be the primary focus in establishing targeted foundational supports.
The absence of supports outside of individualised funding also means that people who do receive individualised funding have an incentive to try and meet all of their needs through individually purchased services. But individualised funding was never intended to meet all of a person’s disability-related needs.174PwC (2009).
And some services, such as information and advocacy services, supported decision-making, or peer support, are not well-suited to a model of individually purchased services. These services would be better delivered as commissioned services available to all disabled people as general foundational supports.
There evidently remains very strong latent demand for support among the more than two million disabled Australians under the age of 65. In the absence of other services, the incentives to push for an NDIS funding entitlement are understandably high. A rebalancing of disability supports is long overdue.
The prevalence of disability is increasing overall, meaning that there will be more pressure on the NDIS in future to cater for more people.175ABS (2024b). With more people with disability needing services, government must find a way to ensure that people who need inclusive mainstream services and low-to-mid-level disability services get access to support in the most efficient way.
A well-resourced and appropriately ambitious foundational supports program will be essential for meeting this growing need, and saving the NDIS from an increasingly unsustainable future.
4.2 Foundational supports should be funded using existing NDIS funds
It is possible to make a serious investment in foundational supports without governments having to find new money. This would meet the needs of a wider population of disabled Australians, while continuing to fund a more targeted system of individualised funding for those who need it most.
We outline a plan to gradually free up funds from individualised funding over a five-year transition from 2026-27 to 2030-31. These funds are freed up by simultaneously:
changing the way certain services are delivered for all disabled people, from purchasing these services with individualised funding under specific line items to receiving these as commissioned services (general foundational supports), and;
changing the way certain groups receive disability services, from receiving individualised funding to either receiving smaller, more targeted individualised funding packages or to receiving commissioned, programmatic services (targeted foundational supports).
Importantly, NDIS funding that is freed up and redirected to foundational supports represents only about 10 per cent of total NDIS payments in the 2023-24 financial year.176Grattan analysis of 2023-24 NDIA payment data: NDIA (2024e). Figure is calculated as the proportion of payments in 2023-24 that were for cohorts and/or service types that would be transitioned to foundational supports under Grattan’s plan.
Pooled together with existing funding for Information, Linkages, and Capacity Building grants and some Partners in the Community funding, this would create a pool of $6.4 billion per year ongoing, from 2030-31, for governments to commission an appropriately ambitious range of foundational supports.
This means that governments can continue to fund individualised NDIS packages and fund foundational supports within the existing NDIS cost projections, without needing to find new money.
4.2.1 We can’t afford to wait for governments to find new money for foundational supports
It is imperative for the sustainability of the NDIS that governments maintain the reform focus on foundational supports and successfully establish a coherent tier of services that can meet the needs of disabled people more effectively and efficiently.
While the federal government and the states and territories agreed in December 2023 to fund foundational supports ‘50/50’,177Shorten and Rishworth (2024). it is not currently clear how this commitment will be met or what quantum of funding is needed.178Federal, state, and territory governments agreed to fund $10 billion over five years from 2025-26, although it is not clear if this funding is intended to cover only foundational supports for children. See State of Victoria (2025, p. 57). There has been little commentary on the implications of this agreement for the NDIS budget, but any strategy that adds costs in net terms does not seem tenable to us.
It is unrealistic and unnecessary for progress on foundational supports to be tied to negotiations on new matched funding from federal and state and territory governments. The many billions of dollars committed by governments to the NDIS can and must be spent more effectively.
If governments decide to find more money to establish foundational supports, there is a risk that they will be little more than a re-badging of existing services, which are inadequate, and this has the potential to exacerbate a worsening postcode lottery of service options available to disabled Australians.
4.2.2 NDIS contributions are already used to fund non-individualised supports
The legislative mechanism already exists for NDIS contributions from the federal, state, and territory governments to be used to fund things other than individualised payments.
Under Sections 13 and 14 of the National Disability InsuranceScheme Act 2013, NDIS funds can be used towards the provision of ‘coordination, strategic, and referral services’, and to fund people or entities to provide information, goods and services, and assistance with capacity building, including for people who do not get any individualised funding. This mechanism is currently used to fund Local Area Coordinators and Early Childhood Partners.
Funds can also be used for early intervention supports for children before their NDIS plan comes into effect – this currently enables the provision of Early Connections and Early Supports to children with developmental concerns.179NDIA (2024i).
This flexibility is reflected in the bilateral agreements underpinning state and territory contributions, which specify that funding ‘will contribute to participant supports’, including both ‘individualised support packages’ and ‘Information, Linkages, and Capacity Building and other general supports’.180NDIA (2022a).
These flexibilities should be employed to enable joint commissioning of foundational supports between the federal, state, and territory governments and the NDIA. Chapter 5 explains how intergovernmental agreements can be used to clarify system interfaces and funding arrangements for the NDIS, foundational supports, and mainstream services.
4.2.3 Rethink the commissioning approach for foundational supports
Establishing foundational supports will require a joint commissioning process between the federal, state, and territory governments and the NDIA. People with disability should also be directly involved in this commissioning process, to ensure that services commissioned respond to their needs.
This would facilitate cohesive management of foundational and individualised supports as two components of a broader scheme of disability insurance. Chapter 5 describes in more detail the features that will be needed for successful joint commissioning of foundational supports.
Organisations commissioned to administer foundational supports should have contracts or agreements for three-to-five years of service at a time, rather than relying on short-term grants. This would give organisations greater certainty to develop and refine supports.181NDIS Review (2023a), Olney et al (2022), and Wilson et al (2021).
Consideration should be given to different methods of securing service provision, particularly in rural and remote areas.182Boer et al (2025). Joint commissioning offers an opportunity to better meet the needs of these communities, where some participants have struggled to access adequate supports under current NDIS funding arrangements.183NDIS Review (2023a, p. 763).
Governments should collaborate with Aboriginal Community Controlled Health Organisations (ACCHOs), and commission them to deliver services that are specific to Aboriginal and Torres Strait Islander people with disability.
Specific approaches could include the use of lead provider contracts with suppliers that can manage a group of sub-contractors, to combine the dual benefits of scaled “back office” and national service consistency with local knowledge and connections.184O’Flynn et al (2014). Relational contracting could also be a valuable tool to enable structured, ongoing cooperation between commissioners and suppliers where services are novel and require the capacity to experiment, innovate and evolve towards formally agreed goals.185Considine et al (2024).
4.3 General foundational supports should be available for all people with disability that need them
General foundational supports is the name the 2023 NDIS Review gave to the first, most basic level of support that should be available to all disabled people. Most disabled people will only need this level of support.186NDIS Review (2023b).
General foundational supports should include:
information about disabilities;
skill development;
self-advocacy and supported decision-making;
educational and parenting programs for parents and carers of people with disability;
peer support;
social and community participation; and
information and referrals to mainstream services and other foundational supports.
In this section we describe the various general supports that should be funded and how, including how existing functions should evolve to support a more cohesive service offering.
4.3.1 Fund information services
Research into ‘Tier 2’ information services indicates that online information about support and services is often out of date or inaccurate, and finding accurate information is difficult and time-consuming.187Olney et al (2022).
Information can help to make the NDIS more sustainable. Easy access to accurate information that tells people which services can meet their needs can help to divert people away from seeking individualised funding in the NDIS.188Ibid.
There should be ‘no wrong door’ for people to access information about disability, local foundational supports, and the NDIS, whether people seek it from government or commissioned services. Information should be available through mainstream services, such as maternal and child health services, GPs, Services Australia, and schools, as well as specialist sites such as the Disability Gateway and from disabled peoples organisations.189Ibid.
4.3.2 Fund individual capacity building programs
Capacity building for people with disability covers a range of essential skills, such as self-advocacy, supported decision-making, exploring housing options,190See Bennett and Orban (2024a). personal care, using public transport, shopping, cooking, forming and maintaining relationships, and social skills.
Research has shown that adults and children with disability benefit from individual capacity building.191Bigby et al (2023).Self-advocacy can also help to safeguard people with disability, especially children, from abuse.192Murphy (2011).
Offering programs that build people’s skills free of charge can also overcome financial barriers facing people with disability and their families.193Andrews et al (2015).
Individual capacity building should also include building the skills required to get and keep a job. Few existing disability employment services focus explicitly on capacity building, instead prioritising downstream interventions such as work placements and job searching.194Kavanagh et al (2021). But capacity building can be critical to success in these activities, and so foundational supports should plug this gap.
This will require careful commissioning, to ensure that these supports supplement and integrate with existing disability employment service offerings.
4.3.3 Give preference to disabled peoples organisations
Governments should give preference to disabled peoples organisations, family organisations, and capacity building organisations in commissioning general foundational supports. These organisations are well-placed to provide information and capacity building services relevant to disabled people, and to advocate for their needs.195Wilson et al (2021).
Historically, these organisations have had patchy and uncertain funding, with several organisations folding through the years, and their expertise is difficult to reclaim once lost.196An example was the closure of Western Australian Individualised Services (WAiS) in 2024.
Research into Information, Linkages, and Capacity Building funding in 2021 indicated that only about half of ILC projects were hosted by disabled peoples organisations and other priority cohort organisations.197Wilson et al (2021, p. 28).
Governments should preference commissioning disabled peoples, family, and capacity-building organisations to provide individual capacity building, education, and programs for families and carers of people with disability.
Governments should also ensure that the range of providers delivering general foundational supports includes organisations with leadership from and expertise in the specific needs of Aboriginal and Torres Strait Islander, culturally and linguistically diverse, and lesbian, gay, bisexual, transgender, queer, intersex and asexual (LGBTQIA+) disabled people.
Disabled people from these groups should be able to access foundational supports regardless of the provider, but targeted commissioning will ensure that services are available, culturally appropriate and able to accommodate their specific needs.
4.3.4 Create a technical hub
Governments should commission a technical hub that would support disabled peoples and family organisations, capacity-building organisations, and any other organisations providing foundational supports.
The hub would be the mechanism that brings these organisations together into a national network, helping to bring consistency to its service offering where that makes sense, such as when implementing an evidence-based approach to peer support.
The hub would be the ‘go-to’ repository of support, resources, and information about best practice, providing a web platform, digital training kits, and a rolling program of communities of practice, training, coaching, and mentoring to share knowledge and encourage improvement. The hub should build the capability of disabled peoples and family organisations, and capacity building organisations, including around leadership, governance, and demonstrating impact.
An Australia-wide collaborative of capacity building organisations, working through a lead organisation, would be well placed to create and run the hub.
Grattan Institute estimates that funding a hub website and a rolling program of training, coaching, and mentoring for disabled peoples organisations and Local Area Coordinators would cost about $3 million to $5 million per year. Funding for the technical hub should come from the broader general foundational supports bucket.
4.3.5 Stacking supports avoids duplication and waste
People with individualised funding should get general foundational supports too; this means any duplicate supports should be taken out of individual plans, because people will be able get them free of charge through local organisations.
Likewise, children with disability or developmental delay and people with psychosocial disability accessing targeted foundational supports should get general and targeted foundational supports at the same time, without duplication across the two categories.
Services that are genuinely different (such as specialised skill development that would not be offered in general foundational supports) should remain in people’s individual funding if they need it.
General foundational supports funding should come with a requirement that services are available to people with and without individualised plans.
And the replacement Section 10 rule we proposed in Section 3.2.4 should be used to ensure that people aren’t purchasing supports using their individualised funding that duplicate those available as general foundational supports.198For more detail on this argument, see Grattan Institute’s submission to the Section 10 consultation: Bennett (2024).
4.3.6 Local area coordination works – there’s no need to start again
Local Area Coordinators (LACs) and Early Childhood Partners are the face of disability services in most Australian communities.199Local Area Coordination, and its early childhood counterpart, Early Childhood Partners, are the two prongs of the NDIS Partners in Community program. They are intended to inform people with disability and their families about the NDIS, how to apply for supports and connect to services, and how to understand and implement their individualised plans.
These roles should benefit both individuals and the NDIS. As well as linking people to services, LACs and Early Childhood Partners are intended to provide the NDIA with valuable insights about service gaps in their communities.
But since the NDIS began, these functions have been poorly implemented, limiting their impact.
Local Area Coordination works best when coordinators can match their time and support to each person’s needs. For many, this could mean brief guidance and referrals to foundational supports. Others, particularly those with more complex needs or individualised NDIS funding, may require more intensive help. But in practice, most coordinators have focused on NDIS participants, leaving little capacity for broader community support, information sharing, and referrals.
Early Childhood Partners have had similar challenges and capacity constraints and have struggled to connect early enough with children and families or sufficiently well with mainstream systems and services.200NDIS Review (2023a).
The 2023 NDIS Review proposed a complete overhaul of the LAC and Early Childhood Partners system, replacing it with a new function – Navigators.201Ibid. The failings in these services are well documented;202NDIS Review (2023a), and Olney et al (2022).however, changes to how they are implemented would be likely to overcome many of the problems, without the need to establish an entirely new system which lacks the established evidence base of Local Area Coordination.203The Review makes other proposals about navigation that Grattan Institute supports; for example, Grattan called for specialist housing and living support navigators to help people with severe disability to design their best housing option. See Bennett and Orban (2024a).
Evidence from Western Australia and the UK suggests there are multiple benefits to people with disability and their families when Local Area Coordination is done well, including:204Bainbridge and Lunt (2021), and Thiery et al (2023).
improved health and well-being,
increased independence,
better access to early intervention,
building social and community networks, and
improved safety.
The original vision of Local Area Coordination, developed in Western Australia and exported overseas, is still possible. As the NDIA brings more of the functions ‘in-house’, coordinators will have more time to spend on referrals, and mainstream and community capacity building for people needing general and targeted foundational supports.
Rather than starting from scratch to design a brand new system of community and mainstream support navigation for everyone, a new Local Area Coordination program should be commissioned which reflects established evidence of best practice, builds on what is working well, and addresses things that have undermined effective implementation to date.
This program should be jointly commissioned with state and territory governments to ensure it is connected to existing foundational supports in each jurisdiction.
4.3.7 The importance of specialised roles for children and families
There is good justification for delineating specialised support and navigation functions for particular groups in the way suggested by the 2023 NDIS Review.205NDIS Review (2023a).
The specific needs of children with developmental delay and disability and their families should be considered when commissioning navigation-type supports. This will ensure that the necessary evolution or replacement of the current Early Childhood Partners program reflects their important future role in linking families to foundational supports and building family capacity, rather than operating primarily as a pathway to individualised NDIS funding and therapy.
The Key Worker model can help families understand their child’s situation, make sense of new information, and navigate and coordinate services options.206Alexander and Forster (2012). These roles will be important in ensuring that new foundational supports for children operate within a supportive, family-centered context that reflects best practice principles in the delivery of early childhood intervention.207Dimmock et al (2024).
4.3.8 How to fund general foundational supports
General foundational supports should be funded from the existing NDIS contributions of federal, state, and territory governments.
By using current funding more strategically – including individualised payments, ILC grants, and Partners in Community contracts – governments can cover the cost of these supports, as well as essential infrastructure such as a technical hub and Local Area Coordination, without needing extra funding (see Figure 4.2).
Grattan Institute has identified $450 million of expenditure in 2023-24 within individualised plans for supports that could be more effectively and efficiently delivered outside of individualised funding as general foundational supports. Notably, this is only about 1 per cent of total NDIS payments for the 2023-24 financial year. This funding is currently spent on 14 line-items, which include:208Note that this analysis excludes funding for self-managed participants, because line-item expenditure data aren’t available for this group. For further detail about this analysis and a full list of line-items, see Appendix A. This analysis is indicative, and the NDIA should undertake a more thorough analysis of expenditure on line-items that could be better delivered as general foundational supports, with a view to further refining this list and funding quantum.
life transition planning, including mentoring, peer support, and individual skill development;
innovative community participation;
school-leaver employment supports;209Note that from July 2024, this line-item is known as ‘Employment Assistance’ in the National Disability Insurance Scheme Pricing Arrangements and Price Limits (see NDIA (2024j)). Grattan refers to school-leaver employment supports because the most recent line-item payments dataset published by the National Disability Insurance Agency is to June 2024 (see NDIA (2024e)).
employment-related assessment and counselling; and
training for carers/parents.
Figure 4.2: Grattan’s proposal for funding general foundational supports
Annual funding for general foundational supports following transition to new funding arrangements, as at 2030-31
Notes: ILC = Information, Linkages, and Capacity Building. PiC = Partners in the Community, including Local Area Coordinatiors and Early Childhood Partners. See Appendix A for further detail about how these numbers were calculated. Source: Grattan Institute analysis.
These services should be provided as foundational supports so that they are available to a broader group of people who would benefit from them, and to avoid inefficient duplication between foundational and individualised supports, for example relating to employment support.210There will still be employment supports available in people’s NDIS plans to provide highly individualised support to people who need it, for example, through ‘Supports in Employment’ which is the largest employment assistance line item by total payments in the NDIS.
This won’t mean fewer services for people currently receiving them. Instead, it reflects a change in how these supports are provided: individualised funding should not be expected to meet every disability-related need, but rather form just one part of a broader system of support.
These line-items should be phased out of participants’ plans starting at their first plan review after 1 July 2026. This should happen gradually over two years, with about 50 per cent of the funding against these line items reduced in the first year, and then 100 per cent reduced in the second year.
Information, Linkages, and Capacity Building grant funding should be better targeted
Information, Linkages, and Capacity Building grants currently span four streams:211Council of Australian Governments Disability Reform Council (2015a).
individual capacity building;
community awareness and capacity building;
information, linkages, and referrals; and
capacity building for mainstream services.
The current funding pool for ILC grants is about $150 million per year.212Commonwealth of Australia (2025b). This funding is delivered as short-term grants to a large number of organisations, with little opportunity for efficiencies from informationor resource-sharing between organisations or regions.213Wilson et al (2021).
These grants are also disconnected from the Local Area Coordination and Early Childhood Partners program (the ILC component of which is funded separately through the NDIA’s operational budget),214NDIA (2024k, p. 55).meaning there is a missed opportunity for oversight and coordination of the total service offering for each region’s population.
Funding from ILC community and mainstream capacity building grants has been spread too thin, and in ways that duplicate government’s responsibilities in these areas under the Australian Disability Strategy. This funding should be redirected to the Partners in the Community program.
Local Area Coordinators and Early Childhood Partners are contracted to help local community and mainstream services to better understand disability and how to become more inclusive. In the future, local area coordinators and organisations supporting children and families will need to help a larger group of people with disability to access general foundational supports. Government should ensure they are freed up to do this work by reducing their planning workload.
Funding from ILC individual capacity building and information, linkages, and referrals grants should continue to fund individual and family capacity building and information services, ideally provided by disabled peoples and family organisations and capacity building organisations, as outlined in Section 4.3.3. This funding should be pooled with the repurposed individualised funding identified above, to provide a more substantial commissioning budget.
These changes should be implemented immediately, from 2025-26, as part of the implementation of the budget measure ‘Support for people with disability’.215Commonwealth of Australia (2025b).
Using this funding to begin commissioning services in 2025-26 will ensure that sufficient services are available to substitute for the reduction in individualised funding for general foundational supports-like services in peoples’ plans from 2026-27.
Partners in the Community funding should be expanded and re-focused
The NDIA currently spends about $600 million each year on the Partners in the Community program.216NDIA (2024k, p. 67).A substantial proportion – up to 80 per cent – of this funding is used for work relating to disabled people with individualised plans, rather than the navigation, community building, and linkage work with other disabled people that will be needed to underpin a successful system of foundational supports. About 20 per cent of Partners in the Community funding is expected to be used for ‘ILC (Information, Linkages, and Capacity Building) activities’.217Productivity Commission (2017, p. 227). This was equivalent to $120 million in 2023-24.
As the NDIA takes more administrative functions in-house, this workload should taper. The NDIA should seize this opportunity to recommission these services to ensure that at least 40 per cent of funding is earmarked for supporting people with disability in the foundational supports ecosystem.
In addition to freeing up these resources, Grattan Institute also proposes that modest additional funding, of about $45 million per year in 2023-24 dollars, should be allocated to fund these navigation, community building, and linkage roles. This funding could be redirected from ILC funding streams as identified in Section 4.3.8.
In 2023-24 terms, this would mean a budget of about $285 million per year for these activities, out of a total budget of $650 million.
Over time, sufficiently funding these functions is likely to mean better allocation of services and a more sustainable NDIS. As foundational supports become established, the functions and funding arrangements for Early Childhood Partners should be reviewed as we suggest in Section 4.3.7 to ensure this service is optimally designed to enable a locally integrated service offering that reflects best practice in early childhood intervention.
4.4 Targeted foundational supports should replace individualised funding for most children with disability
Early intervention for children aged 0-17 with developmental delay or disability should be delivered as targeted foundational supports, not individualised funding (Chapter 2 outlines the failings of the current NDIS early intervention approach).218Grattan’s analysis includes people aged 0-17, whom we refer to as ‘children’ for brevity. This is because targeted foundational supports that are open to people aged 0-17 better align with the school system, and the evidence suggests that integrating support in the settings where children live and learn is best, as opposed to only clinical settings. Replacing early intervention in the NDIS with targeted foundational supports will enable governments to provide better quality early intervention to a larger group of children within the same funding amount.
Delivering early intervention for children with developmental delay or disability will require gradually changing the way services are delivered to children already receiving early intervention supports, as well as redirecting new applicants to targeted foundational supports and away from individualised plan funding in the NDIS. Importantly, this change would affect children in the early intervention pathway of the NDIS, or those who meet the requirements under Section 25 of the Act. The majority of these entrants are children with developmental delay, or diagnoses of less-severe disability.
Children with lifelong and severe disability (that is, children who meet the disability requirements under Section 24 of the Act, rather than the early intervention requirements under Section 25 of the Act) should continue to receive individualised plan funding in the NDIS.
4.4.1 Governments should commission evidence-based early intervention for targeted foundational supports
Research on early childhood intervention shows that engaging children in ‘natural’ settings, rather than clinical environments, is more effective.219Early Childhood Intervention Best Practice Network (2024), Trembath et al (2022b, pp. 13–15), Early Childhood Intervention Australia (2024), and Dimmock et al (2024). Learning in familiar, everyday settings allows children to practise and build on their skills more consistently.220Early Childhood Intervention Australia (2024).
Studies from the US, the UK, and Australia highlight that integrating interventions into the community, where children with disabilities play with non-disabled peers, builds independence, social skills, and friendships.221Dimmock et al (2024), Early Childhood Intervention Best Practice Network (2024), and Andrews et al (2015). It also reduces the risk of violence and abuse.222Murphy (2011).
To achieve this, targeted foundational supports should be delivered through a broad range of settings, including supported playgroups, early childhood education settings, health and community hubs, libraries, and family- and community-led organisations. These services already have strong relationships with families.
By commissioning services, governments can oversee service quality and ensure families don’t have to navigate the complexity of choosing the right programs. Direct commissioning of evidence-based services would encourage providers to offer higher-quality programs and reduce the prevalence of ineffective therapies.223Trembath et al (2021).
Too many or too few services can harm children with disabilities, but it’s hard to determine the right amount of support for each child.224Whitehouse et al (2020, pp. 87–88), and Trembath et al (2021). In a commissioned system, it will be easier to calibrate services, including their intensity, to the individual needs of each child.
Providers should routinely collect outcomes data about children accessing their services to ensure that services are having the intended impact, and work with families to adjust the service intensity as required.
The NDIA should collect outcomes data from a representative sample of children in targeted foundational supports and conduct system-wide evaluations of the targeted foundational supports system. This should include evaluating the quality of service delivery and help determine the optimal quantity of services for the best results.
Children with disability need to be able to receive multiple services and supports, potentially over several years, and depending on their needs. Evidence shows that children who engage in multiple programs over time achieve better results.225Molloy et al (2019), and Andrews et al (2015).
Commission plenty of supports
If the government commissions too few targeted foundational supports for children with developmental delay or disability, they will miss out on early intervention that could reduce the impact of their impairments and equip them to better engage in their family, school, and community life.
Too few services can mean either not enough spots for each service and long waitlists, or everyone getting a little bit of help, but some people getting not nearly enough. Shortages in foundational supports would also probably mean ongoing very high demand for individualised funding for children in the NDIS.
Targeted foundational supports need to be adequate to meet children’s needs. Given that targeted foundational supports are intended to help children at the margin of needing individualised funding in the NDIS, it is likely that some children receiving targeted foundational supports will need more than ‘low-intensity’ interventions.226The Department of Social Services suggested that children receiving targeted foundational supports could get ‘low-intensity’ supports; children receiving targeted foundational supports will have a spectrum of needs and the services and supports governments commission should meet those needs. See Department of Social Services (2024b).
Targeted foundational supports should be a ‘muscular’ program that caters to higher- as well as lower-intensity needs. Federal, state, and territory governments should be ambitious in the scope and quantity of supports they commission, and the outcomes for children they are reaching for, especially as Grattan’s plan allows for a commissioning budget of about $3 billion nationally per year from 2030-31.
There is a strong argument for government investment on cost grounds alone: it costs the same or less to offer services to children with developmental delay or disability through targeted foundational supports, and the outcomes should be the same or better.
But the case for foundational supports is not just about cost; these services will be more accessible, provided in natural settings, and better placed to meet families where they are. They should be funded at the level children need, with attention to both quality and equity.
As more children take up targeted foundational supports, the government should measure the results, test how well funding is meeting the needs of children with developmental delay or disability and their families, adjust the services it commissions and budget accordingly. Governments should carefully assess eligibility for targeted foundational supports to ensure they remain sustainable.
Support families of children with disability
Achieving better results for children with developmental delay or disability requires working with their families too.227Early Childhood Intervention Australia (2024), and Dimmock et al (2024).The evidence shows educating families of children with disability so they can better understand and support their children can be beneficial for children and parents.228For example, Plumtree Children’s Services’ Now and Next program helps parents of children with developmental delay or disability to improve their parenting skills. An evaluation found that parents reported improved wellbeing and capability to achieve goals without relying on professional help, while another study indicated that parents gained a sense of empowerment that was sustained as long as two years after the program. See Moore et al (2018) and Lancaster et al (2024).
Peer support groups for families and carers of children with developmental delay or disability can help.229Bray et al (2017). Family-based and parent-implemented programs can help parents gain skills and confidence that benefit their children.230Wang et al (2016). And support to help families manage stress can also reduce child abuse, trauma and maltreatment.231Murphy (2011), and Aizer and Rebolledo (2025).
Parents of children with disabilities in Australia tend to have poorer mental health, with higher service use and costs compared to parents of children without disability.232Chen et al (2023).
Family capacity building programs should be funded as part of targeted foundational supports, to ensure that children and their families can achieve the best results.
4.4.2 How to fund targeted foundational supports for children
Targeted foundational supports for children should be funded using the same pool of money currently spent on individualised payments for people younger than 18 in the early intervention stream.
In 2023-24, this spending totaled $2.15 billion.233Grattan analysis of unpublished NDIA data. Note that this figure includes expenditure for 18-year-olds – NDIA age bands don’t split out people aged younger than 18. Without reform, we would expect this to grow to $3.8 billion by 2030-31.234We assume that expenditure in this component of the scheme will escalate at the same rate as total expenditure on participant expenses: NDIA (2024a). See Appendix A for further detail on how we have modelled payment growth.
Under our proposal, supports for this group would be commissioned services that grow more slowly at a stable rate of between 3.5 and 4.5 per cent per year – indexed to a weighted average of wage and price inflation and to population growth.
Over time, this would mean the cost of commissioned supports would fall below what would have been spent through individualised plans, delivering real and lasting savings. These savings would be in addition to the benefit of avoiding the need for new funding for targeted foundational supports for these children.
There are also significant administrative savings. In 2023–24, about $77 million was spent on managing individualised plans for children with developmental delay.235Grattan institute analysis of NDIA (2024e). Figure includes expenditure for supports in the registration group ‘Management of funding for supports in participants’ plans’ for participants with global developmental delay and developmental delay. While commissioned services would still require some overheads, removing the need to manage plans and budgets for each child would cut waste and free up funding for frontline programs that actually improve results for children and families.
A managed transition to the new funding arrangements
This transition will need to be carefully managed to ensure that:
children and families don’t face a service gap: there should be sufficient services available through individualised funding or targeted foundational supports, or a combination, throughout the transition period;
children, families, and service providers have sufficient time to prepare;
it is well-coordinated with other simultaneous reforms to the NDIS – most notably, the shift to new framework planning (see Section 3.2.1); and
governments only funds high quality and evidence-based programs, supports, and services.
To achieve these aims, we propose a gradual transition over five years, from 2026-27 to 2030-31.
Governments should begin jointly commissioning targeted foundational supports in 2025-26, with the first services starting from 1 July 2026.
From that date, no new participants younger than 18 should enter the NDIS early intervention pathway. Instead, their early intervention needs should be met through targeted foundational supports.236Note that this proposal does not affect children who are eligible for the NDIS via the disability requirements pathway.
Children already receiving individualised funding under the early intervention pathway on 1 July 2026 should gradually transition to the new system over two years, starting from their first plan review after that date.
Their new plans – aligned with the revised planning framework – should step down funding over two years as their support needs are increasingly met through commissioned services. This gradual tapering of plan funding will mean that government can establish targeted foundational supports so that children have supports to go to as they transition out of the NDIS.
Some children will have pre-existing two-year plans starting just before the transition date. These children will begin transitioning at some stage between 1 July 2026 and 30 June 2028, with the final group completing the move by 30 June 2030.
As children shift to the new model, funding for targeted foundational supports will increase steadily. By 2030-31 – the end of the transition – this commissioning budget will reach $3 billion a year. From then on, this budget should be indexed to a weighted average of wage and price inflation and to population growth, as outlined in Section 4.4.2.237During the transition period, the NDIA’s Annual Financial Sustainability Report projections assume that a small proportion of children currently receiving early intervention supports will reach a point of no longer requiring disability-specific supports from either NDIS funding or targeted foundational supports. We have maintained this assumption, and slightly reduced the quantum of funds flowing into the foundational supports commissioning budget accordingly. See appendix A for further detail about what this means.
4.5 Providing recovery-focused psychosocial supports through foundational supports
Many people with severe or persistent mental illness experience significant and long-term difficulties with day-to-day functioning as a result of their illness.238Harvey et al (2023), and Productivity Commission (2020). In other words, they experience psychosocial disability – and therefore require psychosocial supports to help them live a meaningful life in the community.
There are about 65,000 people with a psychosocial primary disability currently receiving an individualised support package in the NDIS, representing 9 per cent of all people on the scheme.239NDIA (2025d, Table 1). Half of these participants have a primary diagnosis of schizophrenia.240AIHW (2025b).
Supports for this group should be adjusted to reflect a recovery focus, in line with the expert consensus on best-practice psychosocial supports. Targeted foundational supports should provide lower-level, recovery-focused supports for people with psychosocial disability who do not qualify for individualised funding.
4.5.1 The NDIS is falling short for people with psychosocial disability
The introduction of the NDIS has resulted in a substantial uplift in funding for supports for people with severe mental illness.241NDIS Review (2023a, p. 510). This is a good thing: psychosocial supports have historically been underfunded. But this new funding is not being spent as well as it could be.
Targeted foundational supports can rebalance supports and funding across people with psychosocial disability, so that more people get what they need and government can better prevent costs from escalating.
Funding for psychosocial supports in Australia is too concentrated on assistance with daily living supports for a small group of participants receiving individualised NDIS funding.
The 65,000 people receiving NDIS supports for a primary psychosocial disability have an average package size of about $87,000 per year.242NDIA (2025d, Table 1, 14). Of this funding, 83 per cent goes towards ‘core’ supports, including a total of $4.68 billion per year on ‘core – daily activities’ and ‘core community participation’ line items.243Ibid (Table 14).
This concentration of funding is antithetical to evidence about recovery-oriented best practice, and soaks up too much of the funding that could otherwise be spent on providing a broader base of lower-intensity psychosocial supports to people outside the NDIS.
At the same time, nearly a quarter of a million people in Australia with a severe mental illness have an unmet need for some psychosocial support.244Health Policy Analysis (2024).
Individualised funding should not be the main source of supports for all people with a psychosocial disability in Australia. Many people with an unmet need require less-intensive psychosocial supports that would be better delivered through commissioned, programmatic service offerings, rather than individualised funding.
There is an opportunity to repurpose some of the funding currently concentrated within the NDIS to support the mental health system to offer a broader base of targeted foundational supports, while also ensuring that offerings within the NDIS are better aligned with the evidence about recovery-oriented supports.
Funding for psychosocial supports is poorly targeted
The NDIS is providing psychosocial supports in the context of substantial unmet need outside the scheme. A 2024 report estimated that 230,500 Australians aged 12-64 with a severe mental illness have an unmet need for psychosocial support – meaning they need psychosocial supports, but aren’t currently receiving any from either the NDIS or other programs.245Health Policy Analysis (ibid). Note that this figure only includes people with a severe mental illness, and is in addition to a further 263,100 people with a moderate mental illness who have an unmet need for psychosocial support.
The report also estimates the total volume of support provision that would be required to fill this unmet need: 14.07 million hours.246Ibid.
This suggests that much of this group would require either relatively low-intensity or time-limited supports – an average of 61 hours per year for each person with severe mental illness.247Ibid (p. 76).
This analysis also showed that the NDIS is providing psychosocial supports to more people than all other psychosocial services put together: it estimated that 61,600 people with a severe mental illness receive psychosocial supports through the NDIS,248Note that this number includes a portion of people in the NDIS with a psychosocial secondary disability, and is limited to participants with a ‘severe’ mental illness, as opposed to a ‘moderate’ mental illness. compared with 43,700 people with a severe mental illness who receive them outside the NDIS through other government programs.249Health Policy Analysis (2024, p. 77).
A similar analysis in South Australia concluded that, despite substantial unmet need for mental health services, overall expenditure on specialised mental health community support services exceeded need by about $34 million.250McGrath (2023, p. 50). This overspend was driven by expenditure in the NDIS, while virtually all other community mental health supports were substantially underfunded.
Psychosocial supports currently operate on the edge of a funding cliff. People in the NDIS often receive intensive support, while many outside the scheme get little or none. Yet lower-intensity supports could improve quality of life, reduce future support needs, and deliver better long-term results – all while containing costs.251Productivity Commission (2020, p. 830).
Targeted foundational supports offer a way to close this gap. By making lower-intensity supports available to more people outside the NDIS, governments could distribute funding more evenly and prevent need from escalating.
The NDIS doesn’t fund best practice in psychosocial recovery
The concentration of funds within the NDIS isn’t only a concern because it ties up funds that could otherwise be used to support people outside the scheme. Evidence also suggests that the types of support the NDIS funds are poorly aligned with best practice in psychosocial recovery.
Psychosocial supports should assist people to achieve ‘recovery’, an important guiding principle for mental health supports which refers to ‘the establishment of a fulfilling, meaningful life and a positive sense of identity founded on hopefulness and self-determination’.252Rosenberg et al (2019, p. 2).
Recovery in this context doesn’t refer to eliminating mental illness or its symptoms, which would be the purview of the mental health system – instead, it is about the achievement of personal goals, and acknowledges the capacity of people with severe mental illness to live full, contributing lives.253Davidson (2016).
Research shows that effective recovery support focuses on services that help people build social and cognitive skills, while also assisting them to regain control of key areas of their lives, such as housing and employment.254Giummarra et al (2022), and Rosenberg et al (2019).
The evidence doesn’t show that more supports, or more funding for supports, always means better results. There is also no evidence to show that long-term daily living supports are beneficial in supporting recovery, despite this being the major focus of NDIS funding (83 per cent255This figure is the proportion of total funding spent on ‘Core – daily living’ and ‘Core community’ support categories for participants with a primary psychosocial disability in 2023-24: NDIA (2025d, Table 14)) for this group. This led the 2023 NDIS Review to conclude, ‘Current NDIS funding priorities are inconsistent with evidence about the most effective supports’.256NDIS Review (2023a, p. 512).
This finding is echoed by the South Australian unmet needs analysis, which showed that the overspend on mental health supports in the state was driven by NDIS funding for ‘individualised support and rehabilitation for adults’ – meaning, assistance with daily living and social and community participation. It found that funding for these kinds of supports was more than three times higher than the National Mental Health Service Planning Framework estimate of the funding required to meet the South Australian population’s need for these kinds of supports.257McGrath (2023). The National Mental Health Service Planning Framework is a model that provides the best available benchmarks of the mental health care requirements of Australia’s population, based on evidence about epidemiology and best-practice care. It was endorsed by all states and territories in the Fifth National Mental Health and Suicide Prevention plan: AIHW (2025c).
4.5.2 Individualised funding should be more focused on recovery
To fix the misalignment of funding with best-practice principles, the NDIS should use the new planning framework and stated supports to change the balance of supports in NDIS plans for people with psychosocial disability.
This should focus on the majority of this cohort who do not get Supported Independent Living funding. In time, consideration should also be given to the balance of supports for the smaller and more complex group who are receiving this high-intensity support.
This process should aim to reduce the amount of funds being spent on ‘Core – Assistance with Daily Living’ and ‘Core – Assistance with Social and Community Participation’ by 40-to-60 per cent. This range acknowledges that time-limited practical supports should continue to be available, but that these should not be the main or only supports that people receive, particularly after their first few years in the scheme. The reduction in these supports should not be uniform, with changes to individual people’s plans informed by their support needs assessment, as outlined in Chapter 3.
People should be given the capacity building and recovery coaching support they need during the transition to these lower-value plans, to help reduce their dependence on practical supports.
To support this transition, we propose that $200 million each year should be put towards commissioning a bolstered capacity building and recovery coaching program, to be included in NDIS plans for people with psychosocial disability as a stated support. This would be a significant uplift in funding compared to historical levels – in 2023-24, $76 million was spent on psychosocial recovery coaching – and should be funded out of the reduced expenditure on core supports.258Grattan analysis of NDIA (2024e). This figure includes expenditure against psychosocial recovery coaching line items for people with a primary psychosocial disability.
Transitioning people with psychosocial disability to new funding arrangements
Much like the transition for children out of early intervention, the transition for this group to smaller, more focussed individualised funding packages will need to be carefully managed. We propose that this should take place over the period of 2027-28 to 2030-31, with preparation starting from 2025-26.
Psychosocial recovery coaches and/or support coordinators should begin engaging with existing participants with a primary psychosocial disability over the next two years, to prepare them for this transition prior to plan changes coming into effect.
From their first plan review after 1 July 2027, people with a primary psychosocial disability should have their core funding – for both daily living and social participation – gradually reduced over three years.
Because some people will be on two-year plans starting just before 1 July 2027, the transition will begin for different people some time between 2027 and 2029. The final people will complete their transition by 30 June 2031.
From 1 July 2027, people entering the NDIS with a primary psychosocial disability should receive smaller individualised budgets, with a lower share and amount of core supports.
If this transition is implemented well, spending on this group could be reduced by about $1.5 billion per year (in 2023-24 dollars).259Note that this figure, and all figures in our costings, are derived from 2023-24 expenditure data because this is the last full financial year for which expenditure data was available. See appendix A for further details about the costing methodology. These savings can be redirected to fund targeted foundational supports for more people with psychosocial support needs, as well as the enhanced capacity building and psychosocial recovery coaching program for people with psychosocial disability in the NDIS, without any new investment.
A smaller group of about 1,900 people with a psychosocial disability are in the NDIS under the early intervention requirements.260Grattan Institute analysis of unpublished NDIA data. System issues at the NDIA mean that some participants’ access type doesn’t update when they move into the permanent disability requirements pathway. In practice, this means that this number is likely an overstatement. Since no dedicated early intervention pathway for psychosocial disability has ever been developed, it is unclear what supports this group currently receive.
With the removal of the early intervention pathway, this group should undergo eligibility reassessments. Some may remain on the scheme under the disability requirements, while others could have their needs met through targeted foundational supports. For the purpose of our costings, we have assumed that everyone in this group will transfer into the permanent disability requirements pathway and continue to receive individualised funding.
4.5.3 Governments should fund evidence-based, recovery-oriented supports
The specific supports funded as targeted foundational supports should ideally be backed by strong evidence demonstrating that they increase social and community participation, strengthen informal support networks, and/or reduce future support needs. There is limited evidence about the cost effectiveness of psychosocial supports – where this isn’t available, the NDIA should conduct ongoing monitoring and evaluation to build up evidence over time.261Giummarra et al (2022).
Targeted foundational supports should not be limited to low-intensity or time-limited supports. Supports should be commissioned to span a range of intensities and meet the need of people with at least moderate psychosocial support needs who are at the margin of requiring an individualised funding package within the NDIS. People with lower level psychosocial support needs may still benefit from general foundational supports, including peer support.
Based on these criteria, examples of targeted foundational supports that should be funded include recovery coaching, activity-based group programs, such as recovery camps, art and gardening programs,262Killaspy et al (2022). clubhouses,263Clubhouses are a specific model of community mental health program consisting of a member-run organisation based in a physical space – a clubhouse. There is strong evidence for the benefits of participating in a clubhouse for people with severe mental illness, including improved social connectedness and quality of life, increased rates of employment, and reduced hospitalisations: McKay et al (2018). and family interventions – particularly psycho-education for families and supporters of people with psychosocial disability.264Weld-Blundell et al (2021). Targeted foundational supports could also include employment supports where these are backed by strong evidence and don’t duplicate offerings in other service systems.
Gradually building up the commissioning of these supports over the transition period, until 2030-31, will allow time and opportunity for providers to gradually build their workforce and capability. Throughout this period, the actions being undertaken under the National Mental Health Workforce Strategy 2022-2032 will support this sector development.265Department of Health, Disability, and Ageing (2023).
Across all psychosocial supports, there is evidence that peer leadership can improve outcomes and engagement.266Killaspy et al (2022). The 2024 federal Budget included funding to increase the size and skills of the mental health peer workforce; commissioning of targeted foundational supports represents an opportunity to both utilise and further invest in this workforce.267Commonwealth of Australia (2025b).
Supports should be integrated with the broader mental health system
The NDIS has become a significant funding source for people with mental ill-health in Australia. In 2022-23, the $4.3 billion spent on NDIS supports for people with psychosocial disability was equivalent to one-third of all expenditure by Australian governments on mental health services.268AIHW (2025b).
NDIS spending for this group was substantially higher than expenditure on state- and territory-funded specialised community-based mental health care services ($3.2 billion) or on Medicare-funded mental health services ($1.5 billion) (see Figure 4.3).
Yet evidence shows that NDIS psychosocial disability support is poorly integrated with the broader mental health system.269McIntyre et al (2024), and Rosenberg (2017). There is also evidence that the establishment of the NDIS has had negative impacts on the community mental health system, including reducing its ability to retain a high-skilled workforce and reduced service availability for people with severe mental illness who aren’t eligible for the NDIS.270Devine et al (2022), Hamilton et al (2020), and Salvador-Carulla et al (2023).
Best-practice models of care for people with severe mental illness, such as Assertive Community Treatment and Integrated Case Management, provide integrated support to meet people’s psychosocial and clinical care needs.271Kakuma et al (2017).Siloing psychosocial and clinical care in different service systems – the NDIS and the health system – makes it harder to implement these models of integrated care.
Recent machinery of government changes that bring disability and mental health policy into the same portfolio and department – the Department of Health, Disability and Ageing – represent an opportunity to address the disjunctions between these systems and improve service integration.
In negotiating the next National Mental Health and Suicide Prevention Agreement, governments should consider how the NDIS, including foundational supports, fits with the broader mental health system and how funding arrangements for psychosocial support can be used to better enable best-practice, integrated supports.272At the Health Ministers Meeting on 13 June 2025, the federal, state, and territory governments agreed that unmet need for psychosocial supports will be a priority in negotiating the next National Mental Health and Suicide Prevention Agreement: (Department of Health, Disability and Ageing (2025). This would include considering how foundational supports integrate with the intake, linkage and referrals work being progressed through Medicare Mental Health centres, the Medicare Mental Health website and the National Early Intervention Service.273Department of Health, Disability, and Ageing (2024c), and Department of Health, Disability, and Ageing (n.d.).
In commissioning targeted foundational supports, consideration should also be given to how these services can be integrated with other domains in which people with psychosocial disability interact with government, including justice, housing, and employment.
4.5.4 How to fund targeted foundational psychosocial supports
The reduction in expenditure on individualised funding we propose for people with a primary psychosocial disability amounts to about $1.5 billion in 2023-24 dollars.274See Appendix A for an explanation of how we have estimated this figure.
Governments should begin commissioning targeted foundational supports for people with psychosocial disability from 2026-27, with the first services commencing from 2027-28. These services should gradually expand over the period to 2030-31, as more repurposed funds become available.
Figure 4.3: The NDIS has become a major funder of services forAustralians with mental illness
2022-23 government expenditure on mental health services, in the mental health system and in the NDIS
Notes: S&T = state and territory. MH = mental health services. NDIS expenditure includes all expenditure on payments for participants with a psychosocial primary disability. Mental health system includes all mental health-related service expenditure by federal and state/territory governments. Community-based specialised mental health care refers to ‘specialised community and hospital-based outpatient psychiatric services’. Source: AIHW (2025b).
As with the commissioning budget for targeted foundational supports for children, the commissioning budget for targeted foundational supports for people with psychosocial disability will grow at a slower, more predictable rate than individualised funding.
We estimate that by the end of the transition period in 2030-31, governments would have a commissioning budget of $2.2 billion.275This number accounts for the growth of individualised funding in the time before it is removed from people’s plans, and the subsequent indexation of the commissioning budget in line with inflation and population growth. See Appendix A for further detail on this methodology.
This in addition to the $200 million each year from 2027-28 for a capacity building and recovery coaching program, delivered as stated supports within individualised plans for people with psychosocial disability.
Governments should begin the process of jointly commissioning targeted foundational supports in 2025-26, with the first services operational from 1 July 2026.
4.6 Ensure mainstream services are more accessible
The NDIS was never supposed to be the only game in town for disabled Australians. This will remain the case even if the NDIS is rebalanced in the way we have proposed in this chapter to provide foundational supports to a larger group of disabled people.
The NDIS should not be solely responsible for making Australia’s society and institutions more accessible and inclusive. All government services should provide support to people with disability.
Disabled people who use general foundational supports in future, but don’t qualify for individualised funding or targeted foundational supports, should be able to rely on accessible mainstream government services if they need more help.
For example, Medicare and state health services are there for disabled people who need health services and aren’t eligible for more targeted programs. Governments should consider how allied health services that they commission as targeted foundational supports fit with the allied health services available under Medicare care plans.276See the Medicare Benefits Schedule Complex Neurodevelopmental Disorders Rules, noting that only certain children with disability or complex neurodevelopmental disorders are eligible: Services Australia (2024b).
It will be important to guard against the risk that establishing foundational supports results in further cost shifting from other service systems and an open-ended liability for the NDIS to address unmet need in areas beyond its legislated purpose.
In Chapter 5, we show how this can be achieved through stronger governance mechanisms that clarify responsibilities and hold governments to account.
IN THIS CHAPTER
Share
5 A national agreement for a better NDIS
The current governance of the NDIS is too complex, lacks clear accountability, and has allowed the scheme to drift from its original purpose. Without firm boundaries and shared responsibility across governments, the NDIS has become the default system for unmet need, leading to unsustainable growth and over-reliance on individualised funding.
Recent government efforts to curb NDIS growth are a welcome first step. But without deeper structural change, there is a risk that these measures will fall short and contain costs without addressing the root causes of inefficiency and poor outcomes.
To make the NDIS sustainable and deliver better results for people with disability, the federal and state governments need to work together to deliver the policy changes we have outlined in this report: firmer boundaries around who the scheme is for, a more balanced system of supports, and a more targeted system of individualised funding for those who need it most.
This will require new governance arrangements and much stronger coordination across all levels of government. A new National Disability Agreement is needed to formalise roles and responsibilities, strengthen accountability, and ensure that the significant public investment in the NDIS delivers the best possible results within existing budget settings.
5.1 A new National Disability Agreement is needed
The National Disability Agreement is defunct. It was written in 2008, before the NDIS started, so does not reflect this enormous change in the scale of and responsibility for disability services.277Council of Australian Governments (2008).
Australia needs a new agreement that clarifies the role of the NDIS and foundational supports, and the responsibilities of all governments under Australia’s Disability Strategy.
The federal government should work with the states and territories to develop a new agreement reflecting the content and scope recommended by the Productivity Commission in its 2019 report.278Productivity Commission (2019). The agreement should:
include a statement acknowledging governments’ commitment to the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD);
outline the role of the NDIS in providing supports to people with permanent and significant disability;
make clear that the federal, state, and territory governments share responsibility for the NDIS and foundational supports – and make clear their respective funding contributions and joint commissioning responsibility;
enable the National Disability Insurance Agency to develop the policy levers it needs to operate as an insurance scheme;
include a statement that affirms governments’ commitment to clarifying which supports to people in the NDIS are to be provided through mainstream service systems and which are to be provided through the NDIS;
clarify the regulatory and safeguarding responsibilities of federal, state, and territory governments for the NDIS and foundational supports; and
incorporate a strengthened performance framework to improve accountability to people with disability, their families and carers, and to the wider community, with increased data collection to measure results.
The new agreement should be the vehicle through which the billions of dollars already ‘baked in’ for the NDIS over the next four years are invested more efficiently and effectively to meet the needs of disabled Australians.
The agreement should be independently reviewed and updated every five years.279Ibid (p. 2).
5.1.1 The new agreement should outline the funding responsibilities of all governments
The original National Disability Agreement (NDA) set out how governments would fund and deliver disability services, which were mostly then the responsibility of states and territories. It defined who was responsible for what, and linked funding to broad outcomes.280The outcomes anticipated from the 2008 NDA included increased economic participation and social inclusion, people with disability having choice, wellbeing, and the opportunity to live as independently as possible, and families and carers being well supported: Council of Australian Governments (2008, p. 6).
This aspect of the NDA has been superseded by the bilateral agreements that accompanied the introduction of the NDIS. But the problem is that the scope of the NDIS bilateral agreements only covers each government’s respective contributions to the national scheme, rather than all disability services.
Australia’s Disability Strategy does not plug this gap, since there is no specific funding agreement or model as part of the strategy which sets out government funding commitments.281Department of Social Services (2024c).
This leaves the memorandum of understanding between governments outlining the responsibilities of the NDIS in relation to other service systems (known as the Applied Principles and Tables of Support, or APTOS) to do a lot of heavy lifting.282Council of Australian Governments Disability Reform Council (2015b).
As we outlined in Section 2.2, APTOS has not served as a clear and enforceable articulation of system boundaries, let alone a guarantor of each government’s responsibilities for non-NDIS disability services. This has resulted in cost-shifting between governments, with disabled people the losers in this tussle over costs.283NDIS Review (2023a, pp. 135–137).
The recent co-location of disability together with health and aged care provides the opportunity to deal far more effectively with some of the perverse incentives that have persisted across and between systems – with the levers to address interfaces and blind spots between programs more substantially within the remit of a single federal department.284Commonwealth of Australia (2025c, pp. 20–22).
A refreshed National Disability Agreement should take a whole-of system approach to funding responsibilities, updated to include both general and targeted foundational supports. These responsibilities must be clearly defined. The agreement should set out the services it covers, and it should ensure state and territory programs that provide similar supports are strengthened – not replaced – by new services.
As NDIS bilateral agreements are reviewed, they should align with the new NDA. Each agreement should outline the foundational supports to be delivered in that jurisdiction, and how much of each government’s NDIS contribution will be redirected to fund them during the transition.
The updated NDA should also clarify roles and responsibilities regarding when federal or state and territory governments should act as the provider of last resort, under what circumstances, and how this would be accounted for in NDIS funding contributions.285The NDIA is responsible for maintaining critical supports and responding to market failures within the NDIS individualised funding system. This role should be clarified in the new agreement, together with any new arrangements relating to these responsibilities in the context of foundational supports: NDIS Review (2023a, pp. 794–796).
The agreement should also clarify who is responsible for advocacy and carer services, and commit all governments to making mainstream services more accessible to people with disability. This will strengthen links between the NDA, the Australian Disability Strategy, and other intergovernmental agreements on health, education, housing, and Closing the Gap.
5.1.2 Risks need to be shared across governments
The new agreement should include clear principles for how governments share and manage risk across the disability system.
The shift in the balance of spending on disability between different levels of government that occurred after the NDIS was introduced was deliberate, reflecting the greater revenue-raising ability of the federal government.286Productivity Commission (2011, p. 11).
Since then, states and territories have contributed to NDIS costs based on population, with annual increases designed to cover inflation and population growth, but capped at 4 per cent. The federal government has matched these contributions, covered all administration costs, and taken on the financial risk of growth above 4 per cent.287NDIA (2022a).
But with annual NDIS costs frequently growing by about 24 per cent per year on average, this risk has been significant.288NDIA (2024b, p. 62). By 2024, the federal government was shouldering 71 per cent of total NDIS costs.289Productivity Commission (2025, F – Community Services, Table 15A.1).
From 2028, state and territory contributions will rise to a maximum of 8 per cent annually.290Department of the Prime Minister and Cabinet (2023). This change will better align incentives for all governments to manage scheme growth, since any further moderation in growth beyond the current 8 per cent target will result in reduced contributions.
With an increased share of the risk, the states and territories should expect increased influence. That should come through a stronger role in shaping, commissioning, and delivering foundational supports, which are critical to the long-term sustainability of the NDIS and need to integrate well with existing state services.
Yet as currently proposed, foundational supports would sit outside the NDIS, funded separately and managed under different risk settings.291Ibid.
As we stated in Section 1.5.2, this means there is a risk that these supports are never fully implemented, held back by tight budgets and complex negotiations linked to an uplift in funding for public hospitals.
Even if these issues could be overcome, a separate budget for foundational supports would still be the wrong approach. Our proposed model includes a multi-tiered system under a single budget, to align incentives and avoid unintended consequences.
Bringing foundational supports under the main NDIS budget would provide long-term funding certainty, reduce system fragmentation, and ensure all governments have a shared stake in a more balanced and sustainable system.
The new National Disability Agreement should reaffirm shared responsibility for the NDIS across all levels of government, and set policy parameters for risk sharing in the rebalanced system.
It should make clear that foundational supports are an integral part of governments’ combined NDIS investment – providing prevention, early intervention, and capacity building – alongside individualised funding focused more squarely on the needs of people with significant and permanent disability.
5.2 Foundational supports will require shared governance
The success of foundational supports will depend on strong governance and commissioning arrangements that build trust and support collaboration around shared goals.
The NDIS budget we are proposing be used for foundational supports is a pooled fund combining contributions from both levels of government. Shared funding gives all governments ‘skin in the game’, but more needs to be done to reinvigorate the role of states and territories, which has greatly diminished since the NDIS shifted funding and responsibility to the federal government.
To enable joint commissioning of foundational supports, which are aligned with and complimentary to state services in health, mental health, education, and early childhood, current governance arrangements must evolve.
Under the established governance arrangements of the Disability Reform Ministerial Council and alongside existing oversight of individualised funding by the NDIA Board and the Independent Advisory Council, new multilateral governance is needed to drive collaboration between all levels of government.
Figure 5.1: The Grattan Institute governance model for a better NDIS
Source: Grattan Institute analysis.
An NDIS Commissioning Authority should be established, reporting into the Ministerial Council. It would include senior officials from all governments, and oversee a national framework and roadmap for foundational supports. Its role would be to ensure consistent service coverage, improve accountability, and coordinate responses to gaps, particularly in remote areas.
Each state and territory should also have a Commissioning Board. These boards should include officials from relevant departments (health, education, treasury, local government), as well as the NDIA and the federal government. Their role would be to tailor foundational supports to local needs, aligned with existing services, and commissioned in line with the national framework.
5.2.1 Joint commissioning can deliver system-wide benefits
Effective commissioning of foundational supports will require genuine collaboration between all levels of government, at every stage of the process. This is essential to avoid fragmented policy-making, cost shifting, and a loss of focus on improving outcomes for people with disability.
While different governments may lead different aspects of the commissioning process, this should occur within a joint commissioning framework. The federal government should avoid becoming a distant funder and performance manager that leaves the states and territories to handle delivery.
A well-executed joint commissioning approach has the potential to deal with fragmentation across portfolios and to smooth interface issues between disability services and mainstream service systems such as health, aged care, education, and housing.292The 2023 NDIS Review proposed this model for foundational supports: NDIS Review (2023a, pp. 38–40).
Joint commissioning must be a strategic, end-to-end process – from assessing needs and current services, through to securing new services and monitoring the delivery of results.293Addicott (2014).
Long-term commitment from funders, shared goals, and clear roles and responsibilities are conditions for success.294Bates et al (2023, pp. 474–475), and Newman et al (2012, pp. 34–38).
The experience of co-commissioning primary health services provides a useful analogy.295Previous Grattan research identified Primary Health Networks’ (PHNs’) limited purchasing power and small budgets as a share of total sector funding as inhibiting their commissioning role: Breadon et al (2022, p. 61). Foundational supports commissioners will be in a better position to deliver given their clear leadership over and funding responsibilities for this new system. In the best cases, working together across the full commissioning cycle has enabled shared learning, more efficient engagement, better use of data, and stronger joint ownership of results.296PwC (2020), and Dickinson et al (2012).
Our previous research has shown that local intelligence is critical to effective service commissioning.297Bennett and Orban (2024a, pp. 41–42). Each jurisdictional Commissioning Board should begin by mapping existing services and identifying gaps and priorities region by region.298Several jurisdictions have already done work to inform planning around foundational supports, including determining the scope of current supports and services available, together with issues, gaps, and barriers. This work could feed into the system mapping: Parliament of New South Wales (2025).
This system mapping should follow a consistent national method – such as the framework developed by the Australian Public Service Academy – and be documented in schedules attached to each NDIS bilateral agreement.299Australian Public Service Academy (2024).This will help clarify what services already exist, what’s missing, and where foundational supports will be focused.
Assessing need and understanding demand are key early steps,300Dartford (2006, p. 2). but the search for perfect data should not delay action.301This report has identified a funding stream that should be sufficient to meet need, decreasing the up-front requirement to define demand in granular detail as an input to budgetary considerations.
More important is putting in place strong engagement processes that ensure disabled people, and their families and organisations, have a strong voice throughout the commissioning cycle.302See Loeffler and Bovaird (2019) for a discussion on the importance of elevating the voice of intended service users in the strategic commissioning cycle. The intended beneficiaries of foundational supports are in a unique position to articulate their needs and help design services to meet them.303Cameron et al (2018), and Penny and Slay (2014, p. 43). It is critical that people with disability have a voice in shaping the future of the disability services system, including foundational supports.
To make timely progress, governments should use existing co-design mechanisms where possible.304At a national level, this would mean working through the NDIS Reform Advisory Committee (Department of Social Services (2025a)) and the statutory NDIS Independent Advisory Council (NDIA (2023e)), while also utilising state and territory Disability Advisory Councils.
Giving disabled people a genuine stake in regional commissioning will be vital to achieving a more balanced, responsive NDIS.
5.2.2 Balancing national consistency and regional flexibility
The design and commissioning of foundational supports should be a shared responsibility, but with some elements delivered nationally for consistency, and others tailored by states and territories to reflect local needs.
Not everything needs to be centralised, but a nationally coordinated approach in certain areas will help avoid duplication, ensure equitable access, and support quality and efficiency across the system.
Key responsibilities best handled at the national level include:
A national commissioning strategy and transition plan – covering funding flows, minimum service expectations, and preferred commissioning models (e.g. contracts – including formal relational contracts, lead providers, grants, seed funding, or impact investment).
A national minimum data set and reporting framework – including standard protocols for collecting and using data, and consistent performance measures (see Section 5.4.2 below).
Access to expert advice and evidence – drawing on the work of the new Evidence Advisory Committee to inform commissioning and evaluation practices.305As currently conceived, the role of the NDIS Evidence Advisory Committee (EAC) will be to adjudicate on supports and services that will or will not be considered NDIS Supports under the Section 10 Rules. Under our proposals in Chapter 3, these Rules would be replaced, to enable greater flexibility. A far better role for the EAC is to provide expert advice into government commissioning processes for foundational supports, to ensure they are underpinned by the best available evidence: Department of Social Services (2025b).
Commissioning in under-serviced areas – especially in remote areas, where tailored approaches should be co-designed with Aboriginal and Torres Strait Islander communities.306Although this should be coordinated at the national level, the commissioning approach should prioritise local collaboration and relationship building, between levels of government, communities and commissioning bodies, as well as service innovation, which have been shown to enable better outcomes in healthcare commissioning in First Nations, regional and remote communities: Boer et al (2025).
National regulatory and workforce settings – covering workforce planning, safeguarding mechanisms, complaints processes, and enforcement.
Specialised services or infrastructure where a unified approach is more efficient – such as the national hub we proposed in Chapter 4 to support sector capability and capacity building.
Conversely, states and territories should lead on aspects of foundational supports commissioning that require flexibility to meet local needs, priorities, and service systems.
Key responsibilities at the state and territory level should include:
Setting commissioning priorities and timelines – based on local needs, service gaps, and emerging issues.
Service design and engagement – including consultation with people with disability and their families, co-design processes, prototyping, and market testing.
Selecting fit-for-purpose commissioning models – tailored to each service and within the available funding envelope.
Ensuring equitable access – by monitoring demand pressures, identifying service gaps, and targeting support to priority populations.
Managing coordination with existing services – to best integrate newly commissioned supports with existing mainstream and foundational supports-type services.
Overseeing provider performance and quality – in all sub-national service contracts, and including compliance and improvement processes.
These elements should be set out in the new National Disability Agreement so that the roles of each level of government are clear together with defined governance structures, with responsibility for any functions to support the commissioning process clearly attributed, for example the role of the NDIA in providing support to cost modelling.
5.3 Regulatory responsibilities across the NDIS and foundational supports
Effective regulation and safeguards need to underpin reforms to the disability services system.
The NDIS Quality and Safeguards Commission (the Commission) regulates services and supports in the NDIS, overseeing provider registration, monitoring compliance with the NDIS Code of Conduct and Practice Standards, educating providers, receiving and responding to complaints, conducting investigations, and taking enforcement actions.
Grattan Institute has called for changes to NDIS regulation, including the introduction of unannounced inspections of group homes.307Bennett and Orban (2024a), and Bennett and Orban (2024b).
Foundational supports will be a significant new part of the disability services landscape that also need regulation. Even though foundational supports will not be as intensive as supports for people with individualised funding, they will need careful regulation, monitoring, and safeguards to ensure that people with disability are protected and that services are safe and high quality.
5.3.1 Use established regulatory mechanisms for foundational supports
Foundational supports providers should be subject to the existing NDIS Code of Conduct and, where relevant, the NDIS Practice Standards.
We do not recommend mandatory registration for all foundational supports providers. For most general supports, coverage under the Code of Conduct – as already applies to recipients of Information, Linkages, and Capacity Building grants – is sufficient.308State and territory regulators, with the NDIS Quality and Safeguards Commission, should identify which modules of the Practice Standards apply to types of foundational supports, and ensure that commissioned providers complete these modules as part of the commissioning and registration process. See National Disability Insurance Scheme Quality and Safeguards Commission (2025) and National Disability Insurance Scheme Quality and Safeguards Commission (2024).
Some targeted supports providers may need to register with the Commission, particularly if they deliver services not already regulated by a professional body.
The Commission should streamline oversight for providers and workers already covered by other regulators – such as those regulated by the Australian Health Practitioner Regulation Agency (AHPRA). Unnecessary duplication should be avoided.309Bennett and Orban (2024b).
States and territories should manage provider performance in line with their contracts, and ensure compliance and accountability. State governments must have the power to rescind government contracts with commissioned providers, block poor-quality providers or workers, and take legal action where necessary.
The Commission and state and territory regulators should share information about providers, including audit failures, contract terminations, or enforcement actions, to prevent providers barred in one jurisdiction from operating in another.
To do this, provider registration and worker screening should be better integrated.310Provider registration is an NDIS regulation run by the NDIS Quality and Safeguards Commission. Worker screening checks are also an NDIS regulatory measure run by the Commission. The Commission already provides worker screening checks through state and territory screening units. This system should be expanded to include employees of foundational supports providers, with information about workers shared between jurisdictions.
This would have two main benefits. First, it would mean worker screening is portable across and between states and territories. Second, it would be easier for the Commission and states and territories to track and enforce actions against workers who breach standards, regardless of where they operate.
5.3.2 Promote quality and innovation
Promoting quality and innovation should be a core goal of the new National Disability Agreement. Quality should be understood broadly to include quality of life for people with disability and their communities, the quality of services provided under the agreement, and the strength of the workforce delivering them.
The NDA should include specific commitments to improve quality of life for people with disability, their families, and carers.311Productivity Commission (2019).To lift service quality, the NDA should commit governments to setting and enforcing clear standards across both disability-specific and mainstream services. These standards should be developed collaboratively by federal and state and territory regulators.
Workforce capacity building also needs a clearer, shared approach. The National Disability Agreement should clarify the roles and responsibilities across governments to develop the workforce. This includes ensuring there are enough skilled workers to deliver supports across the NDIS, foundational supports, and accessible mainstream systems.312Ibid (pp. 12, 81).
Given that many workers and providers will operate across systems, workforce development should be consistent and portable. A more joined-up system would make it easier for workers to move between roles and avoid duplication in training and regulation.
To support this, governments should integrate provider and worker registration systems where possible, including shared records of professional development and training. This would improve oversight and reduce red tape.
The NDA should also promote innovation. The current system offers little room for experimentation and no encouragement for doing things differently, despite largely untapped potential to explore better use of technology and alternative support methods.
Disability services and supports need to innovate to become more productive and to more effectively meet the needs of disabled Australians. To this end, the NDA should ascribe clear responsibilities on governments to stimulate new ways of working.
Grattan Institute has previously proposed an innovation fund to properly resource trials of alternative support options in the NDIS. This should extend to new services delivered as foundational supports.313Bennett and Orban (2024a).
Individualised funding for services in the NDIS leaves little room for existing providers or new entrants to trial innovation. Likewise, foundational supports will give longer-term funding to providers to run commissioned services; however, innovators will also need short-term funding to trial new services or technology.314NDIS Review (2023a, p. 50).
The fund could follow the model of the federal Health Innovation Fund or the Productivity Commission’s proposed Mental Health Innovation Fund, to ensure timely access to resources that push the boundaries on current approaches in search of greater efficiency and better results.315Council on Federal Financial Relations (n.d.), and Productivity Commission (2020, pp. 1173–1174).
5.4 Establish a performance framework that focuses on outcomes for people with disability
In a flurry of new reforms and outdated agreements, there is a risk of losing sight of how policy changes affect the lives of people with disability. The new National Disability Agreement should include a performance framework as a vehicle for governments to agree on the outcomes that matter.
Existing performance indicators have either expired or are ineffective. The previous National Disability Agreement’s performance indicators expired in 2018, and the Productivity Commission’s 2019 review of the agreement recommended that it be overhauled.316Productivity Commission (2019).
Since then, Australia’s Disability Strategy (ADS) introduced a new outcomes framework.317AIHW (2025a). But the Disability Royal Commission called for changes to the ADS, including better measures of government progress toward fulfilling the rights of people with disability articulated in the Convention on the Rights of Persons with Disabilities.318Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (2023, pp. 86-88, vol. 5).
Governments should agree to a performance reporting framework that replaces both the existing National Disability Agreement performance indicators and the outcomes framework in Australia’s Disability Strategy. Governments should publicly report on their progress against the framework every two years, with reviews of the framework itself every five years.
The new National Disability Agreement needs to track government performance against a clear set of outcomes for people with disability and their families, providers, and the community. Outcomes should link to the NDA’s overarching policy objectives.319Productivity Commission (2019, p. 133).
The performance framework should measure people’s quality of life (results), not only costs or service metrics (inputs and outputs).320Ibid (pp. 132–136).
Performance data should be used to evaluate the effectiveness of policies and reforms in improving the lives of Australians with disability, and whether the policies bring at least as much benefit to society as they cost.
5.4.1 Getting the balance of performance indicators right
Although negotiating shared performance indicators can be a laborious process, it represents an opportunity for governments to clarify their objectives and commit to a shared vision of disability services and inclusion in Australia.
Performance indicators are the bridge between the data and the impact of policies on people’s lives. They should be measurable, achievable, and ambitious, and the indicators should inform policymakers and researchers about the effectiveness and efficiency of disability policies.
Indicators should look at the experiences of disabled people in accessing specialised disability services and mainstream services. Linked data assets, which integrate data on people’s experiences across multiple government systems and surveys, provide a tool for governments and researchers to more fully understand the lives of people with disability and their families. In future, the National Disability Data Asset could be used by governments to support more informative performance indicators.
State and territory governments should maintain their commitment to developing the National Disability Data Asset, including providing the resources and authority to progress data development work and link more data to this asset.321Currently hospital data is only available from SA and the ACT, and other state and territory datasets, such as justice and child protection data, are not available for any jurisdiction, limiting the usefulness of this as a national dataset: AIHW (2025d).
5.4.2 Collect nationally consistent service data
To effectively measure performance, governments must collect data on outputs and outcomes. The NDIA already holds and collects extensive data on people in the NDIS, providers, and payments, which provides a foundation to build upon. But the establishment of foundational supports will require new data development.
Before 2018-19, disability services data were captured in the Disability Services National Minimum Data Set, which is held by the Australian Institute of Health and Welfare. But, funding to collect and maintain this data set lapsed in 2018-19, which coincided with most services transitioning to the NDIS and being captured in NDIA data. As a result, there is no national tracking of non-NDIS disability services.
With the roll-out of foundational supports, a new data set is needed to fill this gap. It should capture all disability-specific services delivered outside of individualised NDIS payments, including both general and targeted foundational supports.
This should take the form of a national minimum data set – a consistent, mandatory set of data items that all governments agree to collect and report.322AIHW (2023). This will provide an enduring, nationally consistent, and high quality source of information for governments and researchers to inform policy, support accountability, and guide future investment.
These data should be comparable to data collected about people in the NDIS, and enable linkage, to follow people who move between these systems. This is because the sustainability of the NDIS is closely linked to the sustainability and effectiveness of the entire disability services system, and vice versa.323NDIS Review (2023a, pp. 1076–1077).
In a system involving multiple governments and many providers, standardised data are essential.
Establishing a national minimum data set will need close cooperation, with governments agreeing on:
the specific data items to be collected at each point of service;
definitions and reporting standards;
the right balance between rich data collection and a manageable reporting burden;
strong privacy protections and public trust; and
opportunities for future linkage to other data sets, such as the National Disability Data Asset.
The new national minimum data set should be agreed on, and the governance and technical infrastructure established, before foundational supports commence on 1 July 2026, to ensure that data are captured from day one.
Evaluate disability services
Robust evaluation is vital to improving the quality and effectiveness of disability services.324Productivity Commission (2019). As foundational supports are introduced, evaluation should begin immediately and continue over the long term. Without it, governments cannot know whether reforms are working — or whether people with disability are better off.
A national evaluation agenda should start now with benchmarking of people in and outside the NDIS, and in particular, children and people with psychosocial disability before they move to foundational supports. The data monitoring and performance framework described in Section 5.4 should underpin ongoing evaluation. Evaluations should test whether funding is adequate to meet people’s needs (including identifying any shortages and their impact on people with disability) and whether supports are delivered efficiently and fairly. Evaluations should assess eligibility for targeted foundational supports to ensure that it remains sustainable.325The transition to establishing foundational supports could also be an opportunity for researchers to conduct natural experiments; governments should facilitate these opportunities as much as possible by collecting data and making them available to researchers.
Because evaluations are resource intensive and often underfunded, the National Disability Agreement should explicitly require governments to evaluate foundational supports and the NDIS throughout the transition period from 2025-26 to 2031-32, and then across the system once reforms are embedded.326For example, the Productivity Commission notes that a lack of resources is one reason for a dearth of coordinated and objective evaluations in the mental health sector in Australia: Productivity Commission (2020, p. 1233).
Federal, state, and territory governments should jointly commission evaluations of foundational supports and the NDIS. They should use a shared set of outcome measures to ensure consistency and objectivity.
These outcomes should focus on what matters: whether people with disability are better able to overcome barriers to social and economic participation.
Governments should also commission cost-effectiveness evaluations to maximise the benefits people receive from disability services and minimise waste – for example, by using best-practice guidelines developed by the UK’s National Institute for Health and Care Excellence.327National Institute for Health and Care Excellence (2012).
IN THIS CHAPTER
Share
6 A new sustainability roadmap
Australia needs a disability support system that delivers for people with disability while remaining financially sustainable into the future. Without further concerted reform, the NDIS will continue to grow faster than governments can afford but without the results to match, putting pressure on public finances and risking the long-term viability of the scheme.
This final chapter outlines the cumulative impact of our proposed reforms to save the NDIS, and their implications for disability spending. Central to our plan is the transition of a modest proportion of individualised funding into a new, ambitious tier of foundational supports – funded within existing government contributions to the NDIS.
This approach rebalances disability services to deliver better results, within existing government budgets and incorporating committed savings targets. It also further moderates NDIS growth beyond those targets and will reduce future demand pressure on the scheme.
Governments should adjust the current reform roadmap, which requires new spending and unnecessarily ties progress on disability reform to parallel hospital funding negotiations. This risks further delay and diverts focus from fixing critical flaws in the design of the NDIS.
Governments should instead adopt our proposals and develop a revised roadmap to deliver a better-targeted, sustainable NDIS that improves the lives of disabled Australians.
6.1 Our plan means a sustainable disability supports system
The reforms recommended in this report would bring the growth rate of the NDIS down to an average of less than 7.5 per cent per year by 2033-34. As outlined in Chapter 4, the key to achieving this growth moderation is to fund foundational supports using existing NDIS contributions, rather than new funding.
Figure 6.1: Our plan would save governments $12b on individualisedNDIS payments and up to $34b on foundational supports over 10 years
Projected NDIS expenditure
Notes: ‘June 2024 NDIS cost projection’ and ‘Government’s current plan, including foundational supports’ are both based on the adjusted baseline, which is explained in Appendix A. Additional expenditure on foundational supports under the government’s current plan has been estimated based on the figure of $10 billion over five years in the 2025 Victorian Budget. See State of Victoria (2025). Source: Grattan Institute analysis. See Appendix A for further detail on our costing methodology, and Appendix B for further detail on how we have estimated expenditure on foundational supports under the government’s current plan.
This shifts some of the fastest-growing participant cohorts to a model where governments can better manage costs. The transition will occur gradually over five years.
During this period, a small proportion of funding, services, and people will gradually shift from individualised funding to foundational supports. This shift equates to a re-purposing of 10 per cent of total NDIS payments.328Grattan analysis of 2023-24 NDIA payment data: NDIA (2024e). Figure is calculated as the proportion of payments in 2023-24 that were for cohorts and/or service types that would be transitioned to foundational supports under Grattan’s plan.
This shift will involve a modest upfront cost – about $300 million between 2025-26 to 2027-28 – but this will be more than made up for through lower expenditure growth by 2029-30, with savings compounding after that.
Once in place, foundational supports will be delivered through a commissioning budget that grows in line with underlying inflation and population growth. This will result in spending on foundational supports rising by 3.5-to-4.5 per cent annually.
At the same time, individualised funding will be more targeted, meaning a less costly scheme than governments presently envisage.
Collectively, Grattan Institute’s plan will save governments $12.1 billion over the decade to 2035-36 (see Figure 6.1).
In addition, using existing NDIS contributions to fund foundational supports also avoids the need for governments to find at least an extra $33.8 billion over the decade to fund general and targeted foundational supports for children, plus an additional amount to fund targeted foundational supports for people with psychosocial disability.329State of Victoria (2025).
6.2 NDIS reform should not be tied to hospital funding
In Chapter 1, we argued it is unlikely that foundational supports will materialise in any meaningful way during this term of federal government without new and different thinking.
Progress on NDIS reform is currently tied to parallel negotiations on an uplift in National Health Reform Agreement contributions from the federal government for state-run public hospitals.330Department of the Prime Minister and Cabinet (2023). This follows the National Cabinet agreement in 2023 to fund foundational supports through a deal that ensures expenditure on combined health and disability reforms will result in all states and territories being better off.
But this agreement is not the best platform to ensure NDIS reform or to navigate fiscal challenges. Uncertainty around future demand and liabilities for foundational supports, together with mounting pressure in the health system, has rendered budgetary assurances hollow and created inertia.
Grattan’s plan enables a more ambitious tier of foundational supports to be established – delivered within existing government contributions to the NDIS – while fixing major design flaws to make the whole scheme more efficient and effective.
The costs of foundational supports should be disentangled from negotiations on hospital funding so that these important areas of government reform can be progressed independently.
6.3 Our reforms must be progressed together
All of the reforms we propose in this report work together to create a sustainable NDIS (see Figure 6.2):
without a stronger ecosystem of foundational supports, a cliff edge will remain at access to the scheme and many disabled Australians will miss out on the support they need;
without clearer eligibility criteria for individualised funding, incentives to get this funding will grow and the uptake of foundational supports will be impeded;
without adopting new budget setting processes to allocate funding based on standardised assessment, plans will remain inconsistent and inequitable with high unit costs and unpredictable inflation.
A new sustainability roadmap should reflect these inter-dependencies and ensure progress with each component of reform while measuring these risks.
Figure 6.2: All our reforms work together to create a sustainable NDIS
Source: Grattan Institute analysis.
6.4 Establish a sustainability roadmap
Governments should commit in the new National Disability Agreement to a further growth moderation target at or below 7.5 per cent by 2033-34. This target should cover the entire individualised funding and foundational supports system, to ensure it doesn’t lead to cost-shifting between these linked systems.
The new agreement should include more than just a target: it should be accompanied by a plan showing how governments intend to get there, how they will monitor progress along the way, and, most importantly, how it will improve the lives of people with disability – a sustainability roadmap.
This sustainability roadmap should start from the clear principle of investment in people with disability that enables their independence and social and community participation as valued citizens in Australian society.
The NDIS Annual Financial Sustainability Report will remain a key tool for monitoring NDIS sustainability.331See NDIA (2024a). But this should be supplemented by reporting requirements around expenditure on and demand for foundational supports, to ensure emerging service gaps and resulting cost pressures are identified and addressed early.
Given that cost moderation in our plan is largely driven by a rebalancing of how services are delivered, particular attention should be paid to how foundational supports and individualised funding are interacting and whether there is a need to further adjust policy settings to get the balance right.
Governments should also explore further opportunities for growth moderation. These should include opportunities for driving innovation in high-cost plans (see Section 3.4) and expanding the use of foundational supports, where this would deliver better outcomes for other groups currently served only through individualised funding.
Allow for cash reserves
To strengthen the NDIA’s ability to manage costs in the individualised funding system, the NDIS should be allowed to build and hold cash reserves – just like any well-managed insurance scheme.
In traditional insurance, providers set aside more money than they expect to spend each year. These reserves act as a buffer, helping cover unexpected increases in claims.
While the NDIS is funded through general revenue and contributions from federal, state, and territory governments – guaranteeing it can meet reasonable and necessary claims – the scheme has consistently exceeded its budget.
In future, governments should not be routinely topping up the NDIS budget. A dedicated cash reserve would give the NDIA Board the flexibility to manage year-to-year volatility – whether from a surge in eligible participants, fewer exits, changes in enterprise bargaining agreements, or an increase in high-cost supports.332Productivity Commission (2017).
It would also provide protection against broader economic shocks or fluctuations in government revenue. And reserves would allow the NDIA to smooth its spending across years, giving all governments more predictability in their contributions and making it easier for them to manage their own budgets.333NDIA (2016c).
The new National Disability Agreement should establish a formal mechanism for creating and maintaining this reserve, including clear rules on how it is funded, drawn down, and replenished over time.
6.5 Implications for the NDIA
The proposals in this report will simplify the administration of the NDIS and reduce the NDIA’s operational workload.
This results primarily from the removal of the early intervention pathway (section 25). A single program design focused on lifelong disability will be far easier to manage and will significantly decrease the number of access and planning decisions required.
Further, as we argued in Chapter 2, our proposals create a more targeted individualised funding system that should enable a long overdue, more concerted focus on driving innovation and improving results for people with the highest needs.
The workforce implications of our proposals to improve claims management and budget setting processes (see Chapter 3) have already been accounted for in previous budget initiatives that funded costs associated with employing needs assessors and designing the new assessment process.334The 2024-25 Mid-Year Economic and Fiscal Outlook (MYEFO) included $280 million to develop a dedicated workforce of NDIS needs assessors: Commonwealth of Australia (2024b).
We expect that some of these budgeted costs will be offset over time through a contraction in the NDIA’s planning workforce as people make their own choices about who supports them with implementing their plans.
Therefore, we do not expect our proposals will impose significant additional implementation costs on the NDIA. We see the NDIA playing a supporting rather than leading role in foundational supports commissioning.
IN THIS CHAPTER
Share
Read our research before it hits the headlines.
Sign up for our latest report releases and our newsletter straight to your inbox.
Sign up now
We change the nation – for good.
Donate to support independent, rigorous, and practical policy research in Australia.
Don't delete me. This is used to get the current Tailwind screen.