Overview
Millions of Australians face an unenviable choice when they need to see a specialist doctor: pay high fees or wait too long for care.
Patients pay a fee for two thirds of appointments with a specialist doctor, such as a psychiatrist or cardiologist. That’s much more often than for the GP, where only one in five visits costs money.
Individual visits can cost hundreds of dollars. It quickly adds up if you need to see many specialists for a chronic disease, such as complex diabetes, or to visit the same psychiatrist many times.
On average, patients who pay a fee are charged $300 a year. Even poor people can face huge costs. One in 10 low-income patients who are billed pay almost $500 a year. The problem is getting worse: fees have soared by 73 per cent since 2010.
Almost a million people delay or skip specialist care because of the cost. They are risking missed diagnoses and delayed treatment. That leads to avoidable suffering and adds pressure on hospitals.
Public hospitals run free clinics, but they provide just a third of all specialist care, and their wait times are often far too long. In many parts of Australia, wait times for urgent appointments are months longer than clinical guidelines recommend.
These problems have festered because the system has been running on autopilot. Governments must tackle five root problems to improve access to specialist care for all Australians.
First, we should train the specialists we need, where we need them. Training places are determined by specialist colleges and the immediate service needs of public hospitals, not the community’s healthcare needs. Too few doctors have been trained in rural areas and in some specialties, such as psychiatry and ophthalmology.
Governments should establish a workforce planning body and tie training funding to its recommendations about what specialist training is needed, and where. While they work on these reforms, governments should make it easier for specialists from comparable health systems to work in Australia.
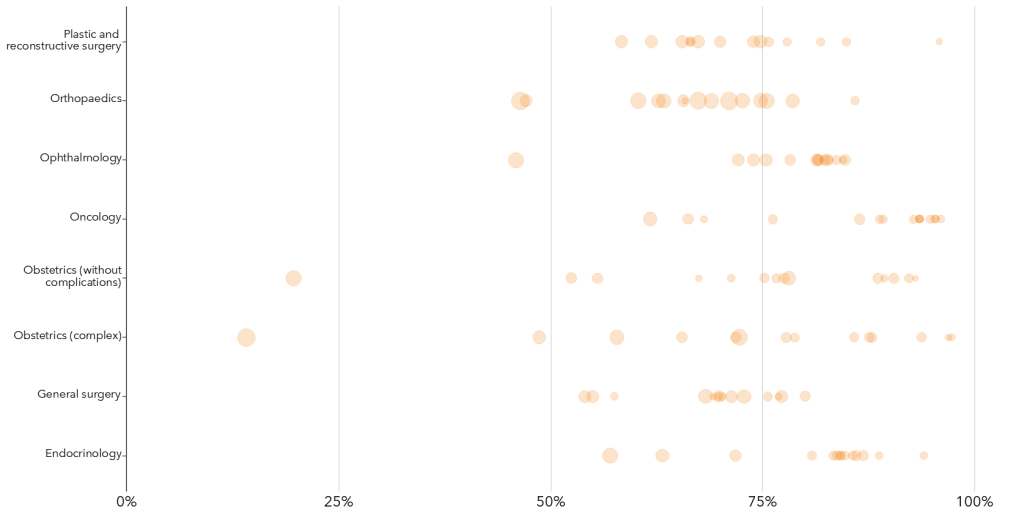
Second, governments should invest more in public clinics, so everyone can get the care they need. Specialist care is a postcode lottery: people living in the worst-served areas receive about a third fewer services than the best-served areas. Public clinics don’t do enough to fill the gaps. Spending $470 million a year would provide one million extra public appointments each year in the areas that get the least care.
Third, to make that investment go further, governments should modernise public specialist clinics, clarifying their role, spreading best practices, and publicly reporting waiting times.
Fourth, governments should take pressure off specialist care by helping GPs manage more care. Systems that allow GPs to easily get advice from other specialists could avoid 68,000 referrals each year and save patients $4 million in out-of-pocket costs. GPs and other specialists would be paid for their time, at a cost of $26 million a year.
Finally, the federal government should combat extreme fees. An initial consultation with a cardiologist or endocrinologist can cost up to $370, and up to $670 for a psychiatrist. The government should claw back public subsidies from specialists who charge extreme fees. This could save up to $170 million a year, and would discourage excessive fees.
There is no time to waste. Without action, fees and waiting times will only get worse as Australians get older and sicker. Targeted investment and sensible reforms will ensure every Australian can get specialist treatment when they need it.
Recommendations
1. Train the specialists Australia needs
- Federal and state governments should establish a national health workforce planning body to set targets for specialist training, including the mix of specialists and the amount of rural training.
- Federal funding for specialist training should be tied to these targets. It should be increased by $155 million a year.
- The federal government should pay specialist colleges an extra $9 million a year to develop and expand flexible training models.
- The federal government should make it simpler for overseastrained specialists to work in Australia.
- Specialist qualifications from more countries with comparable health systems should be recognised.
2. Invest in public clinics where they are needed most
- Federal and state governments should invest about $500 million a year to expand public specialist clinics in areas with the least care.
3. Modernise public clinics
- The National Health Reform Agreement (NHRA) should specify the role of public clinics, and how they will change to provide more and better care.
- States should give public hospital clinics clear guidance on best practices to maximise productivity.
- The NHRA should provide $60 million to spread best practices across the system.
- The independent hospital pricing authority should review specialist clinic funding to make sure prices encourage best practices.
- Federal and state governments should agree to shift current Medicare Benefits Schedule funding to activity-based funding.
- The NHRA should set out a framework for consistently measuring and reporting state and clinic performance.
4. Reduce unnecessary specialist referrals
- Federal and state governments should set up a system that makes it easy for GPs to get advice from other specialists.
5. Reduce extreme fees
- The federal government should withdraw all Medicare funding from specialists who charge extreme fees (fees that are, on average, more than three times the schedule fee).
- The federal government should require referrals to inform patients that they can use a referral to see any specialist, and let them know where to find information about a specialist’s fees.
- The federal government should initiate a review of Medicare Benefits Schedule rebates to ensure they reflect the cost of care.
- The federal government should direct the Australian Competition and Consumer Commission to study specialists’ costs and fees.
Media
IN THIS CHAPTER