Australia should move to blended funding of GPs
by Peter Breadon
Blended funding combines fee for service with flexible budgets to manage a patient’s care over time. It’s used in many countries around the world and has been recommended by Grattan Institute.
Three recent government reviews – the Strengthening Medicare Taskforce Review (2023), the Scope of Practice Review (2024), and the Expert Advisory Panel on the Review of General Practice Incentives (2024) – have recommended it too, so it could be coming to Australia.
If Australia does move to a blended model, it’s important to get the settings right to maximise the benefits to patients, GPs, and government.
Australia overwhelmingly funds GPs through fee for service, where Medicare pays GPs for each patient consultation.
The consequences are well known. Fee for service funding rewards short consultations and low-value care, and doesn’t reward keeping patients healthy. Long wait times and quick consultations are common, while GPs struggle to manage increasing patient complexity.
Fee for service also blocks GPs delegating care to other health professionals such as nurses, pharmacists, or allied health workers. That’s because any delegated care that isn’t funded by Medicare means lost revenue to the GP clinic.
But it doesn’t have to be this way.
Australia’s approach is an international outlier.
Some countries, such as New Zealand, use ‘capitated’ or fixed funding per person. Patients enrol at a GP clinic, which is paid to manage their needs over time. The payment is adjusted up or down depending on patients’ expected needs, and clinics can use it flexibly.
This flips the financial incentives of fee for service funding. Clinics have less reason to provide low-value care, since funding isn’t tied to each visit. It makes prevention pay – if patients get healthier and need less care, the clinic profits. As well, more funding goes to patients with greater needs, making it a fairer way to fund care. And by untying funding from GPs, capitation also gives clinics flexibility to delegate care to a broader team of health professionals.
But fixed funding has downsides too. With a fixed payment, each patient visit takes time but doesn’t bring in revenue. This can lead to clinics providing too little care.
Unless funding is designed carefully, clinics can also game the system by cherry-picking patients with lower needs and avoiding those that would need more care. For clinics, there’s also a risk they lose out when patients end up needing more care than their fixed budget predicted.
Best of both worlds?
Blended funding combines both ways of funding care, and it can be the best of both worlds. But that depends on how much funding remains fee for service, and how much becomes fixed. A new Grattan Institute policy brief shows how to set the right level.
Two competing factors are at play: providing enough fixed funding to make the model financially attractive to GP clinics, but not so much that we lose the benefits of fee for service.
A key goal of blended funding is for GPs to delegate care to a broader team of health professionals. That can help GPs focus on patients with complex needs and reduce wait times. It can also deliver care more efficiently and reduce costs.
But if the level of fixed funding is set too low, it won’t be financially viable for clinics to switch to blended funding and delegate care.
That is because each time a clinic delegates care, they keep the fixed funding but lose the fee-for-service funding. If the fixed funding is too low, it can’t pay for the multidisciplinary team providing the delegated care, or the coordination time to join up care from a bigger team.
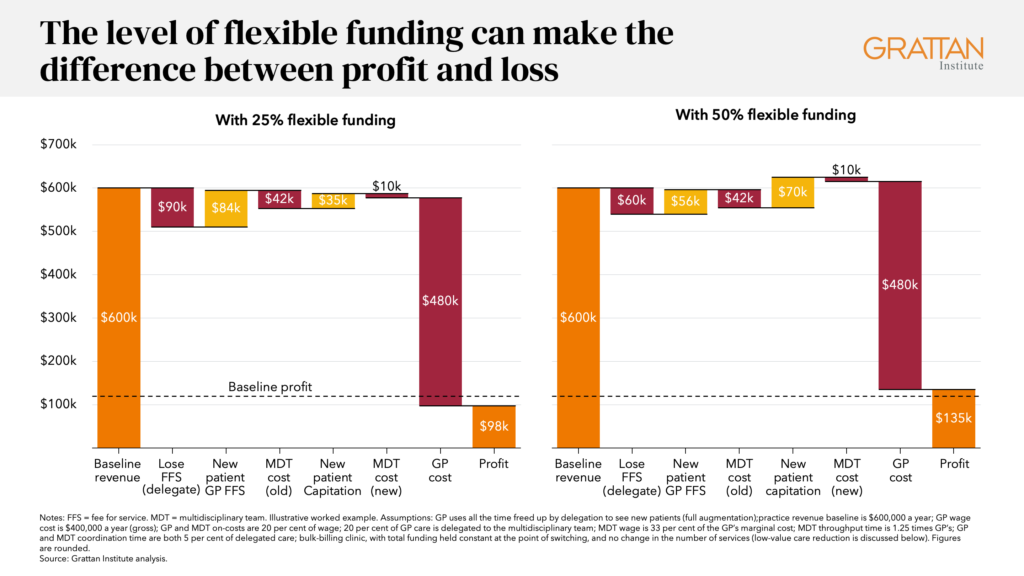
Our policy brief shows an example of a clinic that would make a loss from switching to blended funding if 25 percent of funding was fixed. But when fixed funding rises to 50 percent of the total, switching to the new funding model increases the clinic’s profit.
Risks
But too much fixed funding has risks too. While fixed funding must be high enough to encourage clinics to switch, it shouldn’t be too high.
The risks of fully fixed funding grow with its share of funding. As fixed funding increases, the incentive for GPs to see patient falls, the potential for clinics to game the system increases, and so do financial risks to clinics from unexpected patient needs.
The level of fixed funding also shapes how and when government shares in efficiency gains.
Clinics will delegate care only when it makes financial sense to do so. Our policy brief shows how delegating care can increase profits, particularly if GPs use their freed-up time to see more patients.
Under blended funding, government shares in those gains early. When care is delegated, the government doesn’t pay the fee-for-service part of the funding, so for each visit, it shares in the saving as soon as delegation happens. That could free-up funding to meet rising healthcare demand without stopping clinics earning more than they do today.
By contrast, with full capitation, the only way the government can share in efficiency gains is by changing the fixed funding formula down the track.
So, if the clinic can win, and the government can win, what about the GP?
Retaining some fee-for-service funding keeps a financial incentive for GPs to continue providing direct care to all patients. And the financial incentives of blended funding should see GPs come out ahead.
GPs will be responsible for – and would now get funding for – care coordination and overseeing a broader team.
According to our proposal and the Expert Advisory Panel on the Review of General Practice Incentives (2024), the new funding model should be opt-in. That means clinics that aren’t owned by the GP will need to share financial gains with GPs to bring them along.
Time to get specific
Australia will need to keep increasing funding for general practice as the population grows and ages, but how government pays is important too.
Over-reliance on fee for service fails to match funding and patient need, stops clinics using a broader team of health professionals, and works against fairness, continuity of care, and prevention.
Just pumping in more funding won’t solve those problems. But blended funding can be designed in many ways, and it is time to move from debating whether real funding reform is needed to debating what it should look like.
Discussing specific reform options could help overcome uncertainty and distrust in the sector, and build momentum for an important reform that is decades overdue.
Find out more in our policy brief, The perfect blend: Getting flexible GP funding right.